
Post-Burn Contracture Treatment in Hyderabad | Surgery & Rehabilitation
At PACE Hospitals, a dedicated team of burn specialists, including plastic and reconstructive surgeons, cosmetic surgeons, dermatologists, and rehabilitation experts, manages complex post-burn scars and contractures. Advanced burn contracture reconstruction techniques are used to achieve effective correction, faster recovery, and high success rates. Treatment options include splinting with Z-plasties, skin grafting, flap reconstruction, tissue expanders, and free flap procedures.
Request Appointment for Post-Burn Scar Contracture Treatment
Post Burn Contracture Treatment - appointment
Why Choose PACE Hospitals for Post-Burn Contracture Treatment?

1500+ Z-plasties, Full-thickness skin grafting and local flaps for Post-burn contractures
Team of the Best Plastic and Reconstructive surgeon, Cosmetic surgeon with 20+ years of expertise
Proven outcomes with cost-effective post burn contracture treatment
All insurance accepted with No-cost EMI option
Recognized for excellence in healthcare delivery with
NABH, NABL, NBE/DNB, NABH Nursing Excellence, and ISCCM accreditations.
Advanced Centre for Burns and Post Burn Deformities treatment
PACE Hospitals is one of the Advanced Burns and post-burn deformities treatment hospitals in Hyderabad backed up with plastic and reconstructive surgeon, cosmetic surgeon, dermatologist, functional rehabilitation specialist. Plastic & Reconstructive Surgery department at Pace Hospitals equipped with state-of-the-art facility and latest technology for Skin grafting surgery, burn deformity repair surgery and post burn contracture release surgery.
Post-Burn Contracture
A contracture is one of the complications of burn injury, which occurs when the scar thickness tightens mostly across a joint, resulting in a limitation of movements around the joint. It can also occur in areas apart from joints, like the chest, abdomen, etc., resulting in thickened, hardened, stiff tissue over the body part.

Based on the location, they are classified into:
- Face: Periorbital, Oral, Perioral (Area around the mouth), Nose, Other facial regions
- Upper limb: Axilla, Elbow, Wrist, Hand, Finger, Joints etc
- Lower limb: Groin, Knee, Ankle, Foot, Toes, Joints etc
- Chest
- Abdomen
- Back
- Neck
Based on the severity of the contracture, they are classified into:
- Single linear bands
- Multiple bands
Based on the function involved, they are classified into:
- Completely functional
- Partially functional
- Non-functional
Other classifications are done based on clinical grades and the body areas involved.
Post-Burn Contracture Treatment (PBC)
Post burn contracture (PBC) is treated with the following surgical processes, either alone or in combinations.
- Incisional release
- Excisional release
In a few cases, both procedures are performed, depending upon the severity of the contracture.
Incisional release: It involves incisions on the contracture bands to release the burn contracture. It includes either of the following methods.
- Z-Plasty
- Multiple Z-plasty
- W-Plasty
- V-Y closure
- Modifications of Z-plasty, etc.
Excisional release: It involves the excision of the contracture band or contracted tissue either partially (to safeguard the vital structures) or completely and then covering the wound with any of the following methods, either alone or in combinations.
- Split-Thickness Skin Grafts (STSG)
- Full-Thickness Skin Grafts (FTSG)
- Flaps
- Multiple combinations of the above may be needed in single or multistaged procedures.


Treatment options for post-burn contractures
- Split-skin grafting
- Local plastic surgical procedures: Z-plasty, W-plasty, Y-V plasty
- Full-thickness skin grafting
- Flap cover
- Artificial skin substitutes
- Tissue expansion with or without flap cover
Split-skin grafting
This is an old technique where your doctor will import healthy, unblemished, non-bulky skin without compromising nearby tissues to the defect area. The ideal locations for the graft are the buttocks or scalp. The graft will be applied to the wound once the contracture is completely released and the joint has fully extended.
There are chances of recurrence in this procedure, as the wound will contract once the split-skin graft is placed on the wound bed. This procedure might require physiotherapy in order to prevent movement difficulties, especially in children.
Local plastic surgical procedure
When there is a formation of bands in the contracture, your doctor might use a local procedure in order to release the burn contracture through any of the following procedures.
Z-plasty: It is a procedure that separates the scar contracture and lengthens the band. In this procedure, your doctor borrows tissue from the area next to the contracture rather than growing new tissue to stretch the band. This procedure will be applicable when the contracture is small and there is a good lot of slack skin near the contracture.
The Z-plasty is of two types:
Z-plasty-in-series (example, five-flap Z-plasty)
- The Z-plasty-in-series required a lot of the surrounding tissue.
- The design of Z should always be as large as possible. The bigger the size, the greater the lengthening obtained.
Z-plasty-in-parallel (example, multiple single Z-plasties)
- The Z-plasty-in-series requires less surrounding tissue compared to the Z-plasty-in-parallel.
- The lengthening that is really attained is significantly less.
The benefits of this method are:
- Z-plasty can increase the length of a scar via contracture release in burn contractures.
- In the case of facial scars, Z-plasty has the ability to break up face scars and shift their direction, which enhances the cosmetic outcome.
- Z-plasty can be useful in emergencies. For example, for a hand contracture, Z-plasty can increase the function and range of motion, helping to prevent contractures.
W-plasty: In this method, numerous triangles (like a series of w's) are sliced along the scar's long side and then mirrored on the opposite side. These zigzag patterns produce an irregular broken line when sutured, which reflects light poorly and obscures the original scar.
The benefits of this method are:
- The planning and execution of the W-plasty procedure is simple.
- Minimal risk, as the W-plasty flaps are not transposed, so there is no chance of flap necrosis.
- This approach is particularly useful for scars that occurred on a curved surface, such as the jaw, due to the small size of the flaps and transverse mobility.
- By breaking the scar borders into smaller triangular segments and redirecting the forces that cause contracture, changing the lines of distraction from perpendicular to oblique, and by relieving the bowstringing effect of linear scars, W-plasties may contribute in the improvement of previously hypertrophic scars.
- W-plasty achieves a camouflaging effect by dividing the scar into very small segments and mixing them with normal, unscarred skin.
This procedure is not applicable to certain areas of the body where a certain width of tissue must be given up in the revisional procedure.
Y-V plasty: This procedure is useful for linear sheet contractures. The Y enters the regular skin, and the V runs the entire length of the band. To create a V, the flaps are simply pulled forward. The skin laxity should be enough for the formation of V.
The benefits of this method are:
- There is a low risk of flap tip necrosis since there is no need for undermining, which lessens the possibility of the flaps' blood supply being compromised.
- Scar tissue is reoriented as a result of this technique.
- The length of the contracture band is not important. This technique is helpful with really long contracture bands.
- The Y-V plasty is an easy procedure. It is possible to refine the flap advancement degree while the procedure is being done.
It is actually impossible to remove a thick scar band, and the cosmetic results are very poor.
Full-thickness skin grafting
Full-thickness grafting has a better texture match than split-skin grafting after the contracture has been released, and it also has a lower rate of recurrence. Because there is more dermis in a full-thickness graft, there will be less wound contraction.
Full-thickness grafts are impractical after severe burns because there may not be enough skin to spare. A healthy donor site is required for full-thickness grafts in order for them to enter and exit. This process frequently causes hyperpigmentation, which has poor cosmetic effects.
Flap cover
There are two types of flaps covers:
- Pedicled flaps
- Free flaps.
Both are local and free fasciocutaneous flaps (a tissue flap, which consists of skin and underlying tissues, including a collagen-rich lining tissue, fascia), which are successfully used to relieve the burn contracture.
There is a wide variety of flap choices, which allows the surgeon to make judgments according to each individual case. Local pedicled laps are occasionally ineffective in extensive burn areas due to a lack of local skin plasticity or simply a paucity of available or suitable donor locations. In such cases, your doctor will opt for a free flap.
The size of the free flap should be similar to that of the defect area. Free flap might provide you with an unacceptable cosmetic result as they import tissue which is different in colour, thickness, and texture. There is no chance of recurrence in flap covers, which is the key factor.
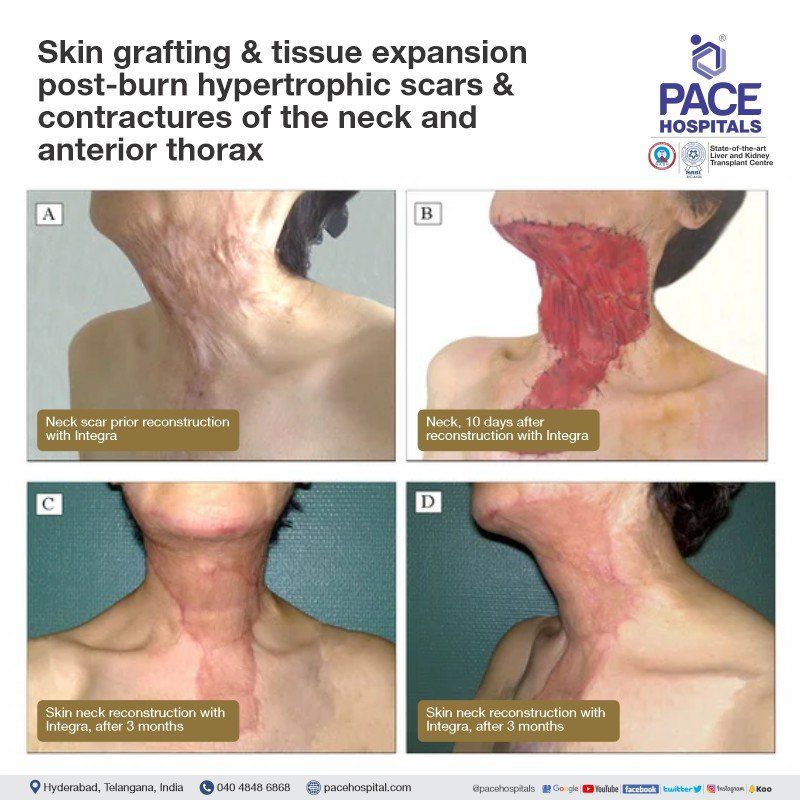
Artificial skin substitutes
These are bilayer artificial dermis products that consist of a porous bovine collagen spongy matrix combined with an overlying temporary epidermal substitute comprised of a silicone sheet (Example: Integra). It reduces contraction by reducing the inflammatory responses.
- The quality of an artificial skin substitute resembles that of a full-thickness skin with improved flexibility and suppleness.
- No presence of scar hypertrophy.
This procedure has a high cost and more intensive dressing requirements.
Expansion of tissue with or without flap cover
It is a simple procedure where the colour, texture, and thickness of the expanded skin are the same as the adjacent skin. In a burn contracture, these tissue expanders are used in combination with pre-expanded or a fasciocutaneous flap. The neck, chest, and scalp are the ideal sites for tissue expansion procedures.
It will be challenging for your doctor to treat burned extremities in the lower limb with tissue expanders. The risks associated with these expansions include infection, leaking, skin ischemia, and even failure. In order to minimise the rate of complications, you should go to routine follow-up appointments.
General principles of burn contracture release
- Prior to distal contractures, proximal joint contractures should be released by your doctor. For instance, if the shoulder and elbow have a restricted range of motion, then there will be little value in having a mobile wrist.
- Each joint should be taken into account independently. If there are several joints that need to be released, each contract should be completely released. Your doctor might opt to use the Y-Vplasty method to release contractures in multiple joints.
- Your doctor will always prioritise function over cosmesis; it is preferable to have a functional joint with a disappointing cosmesis than to have a joint that cannot move but is cosmetically perfect.
- When split-thickness grafts are placed over a wound, they have the potential to form recurrent contractures.Therefore, your doctor might arrange physiotherapy sessions that help to mobilise the joint in order to avoid this. An alternative to split-skin grafts is a flap that has its own blood supply, which could result in an improved cosmetic look.
- The critical underlying structures may occasionally become visible and call for release. For instance, if the ankle joint is released dorsally, it exposes the extensor tendons.
Post Burn Contracture Treatment Cost in Hyderabad, India
The cost of Post Burn Contracture Treatment in Hyderabad generally ranges from ₹5,000 to ₹1,80,000 (approx. US $60 – US $2,160).
The exact treatment cost varies depending on the severity of the contracture, area involved (face, hand, neck, limbs), type of procedure required (physiotherapy, splinting, skin grafting, contracture release, flap surgery), diagnostic evaluation, anesthesia, specialist consultation, hospitalization needs, and overall medical facilities — including cashless options, TPA corporate tie-ups, and assistance with medical insurance wherever applicable.
Cost Breakdown According to Type of Post Burn Contracture Treatment
- Consultation + Initial Assessment – ₹5,000 – ₹8,000 (US $60 – US $96)
- Physiotherapy & Splinting Sessions – ₹1,000 – ₹3,000 per session (US $12 – US $36)
- Basic Blood Tests & Pre-Surgery Evaluation – ₹1,500 – ₹4,000 (US $18 – US $48)
- Minor Contracture Release (Day-Care Procedure) – ₹15,000 – ₹35,000 (US $180 – US $420)
- Skin Grafting Surgery – ₹30,000 – ₹75,000 (US $360 – US $900)
- Z-Plasty / Local Flap Reconstruction – ₹45,000 – ₹1,20,000 (US $540 – US $1,440)
- Contracture Release with Skin Substitute / Advanced Reconstruction – ₹80,000 – ₹1,80,000 (US $960 – US $2,160)
- Hospital Admission (1–3 Days) – ₹8,000 – ₹25,000 (US $96 – US $300)
- Post-Surgery Physiotherapy & Rehabilitation – ₹1,000 – ₹3,000 per session (US $12 – US $36)
Frequently Asked Questions (FAQs) Post-Burn Contracture
What causes contractures in burns?
Contractures are the sequelae of burns depending upon the type and depth of burns, the area involved and the immediate management after burns.
What is done in Post burn contractures?
When a patient visits a plastic surgeon for the treatment of Post burn contracture:
- Thorough functional assessment is done.
- Thorough cosmetic assessment is done.
- Plan of surgery is documented as either incisional release or excisional release or both in combination with an appropriate cover of the wound as required in single or multistaged procedures.
- Postoperative compression garment as required.
- Postoperative splints are planned if needed.
- Postoperative physiotherapy is planned as required.
Which Is the best hospital for Post Burn Contracture Surgery in Hyderabad, India?
PACE Hospitals, Hyderabad, is one of the most trusted centres for treating post burn contractures affecting the face, neck, hands, joints, and limbs.
We are associated with expert plastic surgeons, reconstructive specialists, and physiotherapy teams providing comprehensive evaluation and tailored treatment for:
- Mild soft-tissue contractures
- Severe joint-restricting contractures
- Functional deformities
- Cosmetic and functional limitations
- Pediatric and adult burn sequelae
We provide top-notch facilities such as advanced operating theatres, microvascular reconstruction support, scar management therapies, physiotherapy units, and post-operative rehabilitation, PACE Hospitals ensures safe, effective, and patient-focused treatment — supported by cashless insurance, TPA tie-ups, and complete documentation assistance.
What to expect after surgery in Post burn contractures?
Improvement in function and cosmetic appearance. However, your doctor might give the priority for function before cosmesis as having a functional joint or area is more important than disappointing cosmesis.
Can you reverse contractures?
Yes, contractures can be reversed when they have recently developed. However, contractures may substantially be corrected in months or even years after they first appear.
What Is the cost of Post Burn Contracture Treatment at PACE Hospitals, Hyderabad?
At PACE Hospitals, Hyderabad, the cost of post burn contracture treatment typically ranges from ₹4,500 to ₹1,60,000 and above (approx. US $55 – US $1,925), offering an affordable and specialized option for reconstructive and functional recovery. However, the final cost depends on:
- Type and severity of contracture
- Area involved (face, neck, hand, elbow, knee, etc.)
- Need for skin grafting or flap reconstruction
- Hospital stay and anesthesia requirements
- Physiotherapy and long-term rehabilitation
- Plastic surgeon’s evaluation and complexity of surgery
- Co-existing complications such as infection or scar hypertrophy
Milder cases managed with physiotherapy and minor procedures fall in the lower range, while complex contractures requiring advanced reconstructive surgery fall on the higher end.
After clinical evaluation and imaging (if required), our plastic and reconstructive surgery team provides a personalized treatment plan and a transparent cost estimate based on your functional goals and clinical needs.
How do you treat a burn contracture?
The choice of non-surgical or surgical approach depends on location, extent and degree of contracture. Burn contractures can be treated with Z-plasties to release contracting bands, incisions and skin grafting or excision and resurfacing with skin grafts, artificial skin substitutes, local rotation flaps, tissue expanders with or without free flap.
Who are more prone to develop contractures?
The patient needs to visit a plastic surgeon after any burn injury. If the initial management of a burn patient is done by a plastic surgeon, it significantly reduces the severity of contracture compared to if it is done by any other doctor.
How do you prevent contracture from a burn?
- Wearing a splint across the joint keeps the burn part straight, which helps in the prevention of contracture.
- Through performing range of motion exercises and regular exercises.
- Encouraging daily activities like dressing, clothing, brushing, bathing, etc.
- Applying scar modification treatment protocol as per the plastic surgeon.
- How long does it take for contracture to develop?
- It depends upon the type of burn injury, the extent of burns, depth of burns, location and various other factors. However, you can minimise the formation of contracture by consulting a plastic surgeon after any burn injury.
Do I need to wear a compression garment?
Yes, your doctor might insist on wearing a compression garment. It protects your healing incisions from bacteria, improves your circulation, reduces pain or bearable when you cough, laugh or sneeze.
How long do I need to wear compression garments?
Plastic surgeons recommend wearing a compression garment throughout the day (it can be removed while having bath) for the initial 9 to 12 months, which might vary from a case-to-case basis, as it depends on the surgical procedure and extent of the patient's contracture. After around one year, depending on the patient's progress, the plastic surgeon might change the duration of wearing the compression garment from 24 hours/day to 12 hours/day for variable months.
What is the role of physiotherapy in Post burn contractures?
Physiotherapy plays a crucial role in the management of post burn contractures. Depending on the severity, it starts from day one after surgery and continues for months to years (in some cases). It helps to improve function and maintains the attained position after Post burn contracture surgery. In some cases, it might help to increase the range of motion.




