
Inflammatory Bowel Disease (IBD) Treatment | Diagnosis & Cost
Renowned as the best hospital for IBD treatment in Hyderabad, India, PACE Hospitals provides expert care for patients with IBD disease. Our team of IBD specialists ensures accurate IBD diagnosis using advanced IBD tests, followed by tailored treatment plans. Through innovation, compassion, and medical excellence, we aim to deliver optimal results and support a possible IBD cure.
Book Appointment for
IBD Treatment
IBD Appointment Enquiry
Why Choose PACE Hospitals for IBD Treatment?

State-of-the-Art IBD test & diagnosis Facilities
Best IBD Specialists in Hyderabad, India
24/7 Emergency Gastrointestinal & Inflammatory Bowel Care
Affordable & Reliable Medical & Minimally Invasive IBD Treatments
Recognized for excellence in healthcare delivery with
NABH, NABL, NBE/DNB, NABH Nursing Excellence, and ISCCM accreditations.
Inflammatory Bowel Disease (IBD) Diagnosis
Early diagnosis and effective treatments are key to manage inflammatory bowel disease (IBD) and reduce its impact on patients’ quality of life. Understanding the diagnostic methods and treatment strategies can help both healthcare experts and patients take informed steps to manage IBD.
The diagnosis of inflammatory bowel disease involves:
- Medical history
- Physical examination
- Laboratory tests
- Specialized imaging techniques
Because IBD has symptoms that overlap with other gastrointestinal disorders such as infections or irritable bowel syndrome (IBS), a thorough diagnostic process are required to confirm the existence of the disease and rule out other conditions.
The treatment of inflammatory bowel disease, on the other hand, is aimed at reducing inflammation, controlling symptoms, preventing flare-ups, and improving the patient's overall well-being. While there is no cure for IBD, current therapies can significantly help manage symptoms and reduce the frequency and severity of flare-ups.
The first step in diagnosing IBD is a detailed medical history and a thorough physical examination. Since the symptoms of IBD—such as abdominal pain, diarrhea, fatigue, and weight loss—are nonspecific, it is important for the clinician to gather comprehensive information to differentiate IBD from other conditions.
Medical history
The first step in diagnosing IBD is obtaining a complete medical history. This is an important step in the diagnostic process since it provides context for the patient's symptoms. The Gastroenterologist may ask questions about the onset, duration, frequency, and severity of the symptoms, particularly focusing on common IBD signs such as abdominal pain, diarrhea, blood in the stool, and unintended weight loss. Understanding when these symptoms begin, how often they occur, and how they have progressed over time helps in forming a differential diagnosis.
The gastroenterologist may also inquire about a family history of gastrointestinal diseases, particularly IBD. As there is a genetic component to IBD, a family history of conditions like Crohn's disease or ulcerative colitis can significantly increase the risk of developing the condition. As IBD is an autoimmune condition the gastroenterologist may also take a relevant family history.
A thorough review of the patient's medications is also done, because certain class of medications, like nonsteroidal anti-inflammatory drugs (NSAIDs), can cause or worsen the symptoms of IBD.
Furthermore, the patient's travel history plays an important role in ruling out diseases that can mimic IBD, particularly in cases of traveler’s diarrhea or parasitic infections.
The gastroenterologist, also gathers information regarding the patient's general health status, including any previous gastrointestinal issues, such as recurrent infections, history of abdominal surgery, or previous diagnosis of irritable bowel syndrome (IBS). The patient's lifestyle, including stress levels, alcohol consumption, and smoking habits, are also discussed, as these factors may influence the severity of symptoms and flare-ups in IBD.
Physical examination
Physical examinations are a crucial part of the diagnostic process and often provide the first visible signs that something is wrong. The physician will begin by assessing the patient's general health and appearance. Patients with IBD may appear ill, with signs such as pallor (suggestive of anemia), fatigue, or malnutrition, particularly in cases of severe disease.
The health care expert may then proceed to inspect the abdomen for signs of distention or bloating. Abdominal palpation helps detect tenderness, masses, or areas of rebound tenderness, which could indicate inflammation, abscesses, or bowel perforation. If the patient has an inflamed or obstructed bowel, localized tenderness might be more prominent.
A physical exam also includes an assessment of the perianal area. In patients with Crohn's disease, perianal fistulas or abscesses may be present. These are often significant signs of the disease, as Crohn's disease can affect any part of the gastrointestinal tract, including the perianal region.
The health care expert may also assess extraintestinal manifestations, such as joint pain, skin rashes, or eye inflammation, which are more commonly seen in patients with IBD, especially those with Crohn's disease. Systemic signs such as fever, and tachycardia (increased heart rate) may be present during acute flare-ups or active diseases.
Laboratory tests
Laboratory tests are a fundamental part of diagnosing IBD and are often performed early in the diagnostic process to provide evidence of inflammation and rule out other conditions.
A complete blood count (CBC) is typically performed to look for anemia, which is common in patients with IBD due to blood loss or malabsorption. A complete blood picture may also reveal elevated white blood cell (WBC) counts, which can indicate infection or inflammation. Platelet counts may also be elevated in active disease.
C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are two common inflammatory markers that are often elevated in IBD. These markers do not specifically diagnose IBD but serve to indicate the presence and extent of inflammation. Elevated CRP levels are particularly useful in identifying acute flare-ups.
Fecal calprotectin is another important lab test. It is a protein seen in the feces that is commonly increased in IBD, indicating intestinal inflammation. This test is non-invasive and can help differentiate between IBD and other conditions, such as irritable bowel syndrome (IBS), which may present similar symptoms.
Other stool tests can help rule out infections, especially in patients with diarrhea, by looking for bacterial pathogens, parasitic organisms, and Clostridium difficile toxin. These tests are critical to confirm that the symptoms are due to IBD and not an infectious cause.
In some cases, a serologic test can be used to detect specific antibodies. For example, in Crohn's disease, patients may have anti-Saccharomyces cerevisiae antibodies (ASCA), while patients with ulcerative colitis may test positive for perinuclear antineutrophil cytoplasmic antibodies (p-ANCA). However, these tests are not diagnostic on their own and are usually used to support the clinical picture.
Imaging techniques
Imaging techniques are important diagnostic modalities to diagnose and monitor IBD. These methods help visualize the extent of disease, complications, and areas of inflammation that are not apparently identified through physical examination or laboratory tests.
One of the primary imaging techniques is colonoscopy, which remains the gold standard for diagnosing IBD. This procedure allows visualizing the colon and rectum directly, helping to characterize the signs of IBD, such as bleeding, ulcers and granularity of the mucosa. Biopsies taken during colonoscopy can provide crucial histological evidence to differentiate between Crohn's disease and ulcerative colitis.
In patients with suspected Crohn's disease, which may affect areas beyond the colon, upper endoscopy (esophagogastroduodenoscopy) may be used to examine the stomach and duodenum. This is especially important in cases where the disease is suspected in the small intestine or upper GI tract.
In addition, capsule endoscopy, in which a patient swallows a small camera that transmits images as it travels through the GI tract, is particularly useful for diagnosing small bowel Crohn's disease, which may be difficult to visualize with traditional endoscopic methods.
For more detailed imaging, advanced techniques like computed tomography (CT), enterography and magnetic resonance imaging (MRI) are recommended, as they provide high-resolution images of the small intestine are recommended. These imaging studies are useful for identifying strictures, abscesses, and other complications of Crohn's disease. These techniques can also assess the extent of the disease, particularly in Crohn's disease, which often affects areas beyond the colon.
For more acute cases, an abdominal X-ray may be performed to detect bowel perforation, obstructions, or toxic megacolon, which can be life-threatening complications of IBD. Ultrasound can also help evaluate abdominal pain or complications like abscesses, particularly in patients with Crohn's disease, as it is a non-invasive and cost-effective imaging option.
Lastly, in the case of severe disease or extraintestinal manifestations, additional imaging studies may be ordered to evaluate complications in the joints, skin, or eyes, especially if patients present with symptoms suggestive of extraintestinal manifestations of IBD.
✅Inflammatory bowel disease (IBD) differential diagnosis
The differential diagnosis of Inflammatory Bowel Disease (IBD) includes conditions that present similar gastrointestinal symptoms. Proper differentiation is essential to ensure accurate diagnosis and appropriate management, as these conditions may share overlapping symptoms but require distinct therapeutic approaches and have varying prognoses.
The differential diagnosis of Inflammatory Bowel Disease (IBD) includes conditions such as:
- Anorexia Nervosa
- Appendicitis
- Clostridioides (Clostridium) Difficile Colitis
- Microscopic Colitis (Collagenous and Lymphocytic Colitis)
- Cytomegalovirus (CMV)
- Cytomegalovirus Colitis
- Diverticulitis
- Eosinophilic Gastroenteritis
- Food Poisoning
- Bacterial Gastroenteritis
- Bulimia Nervosa
- Intestinal Motility Disorders
- Intestinal Radiation Injury
- Irritable Bowel Syndrome (IBS)
- Lactose Intolerance
- Salmonella Infection (Salmonellosis)
- Viral Gastroenteritis
- Celiac Disease (Sprue)
- Giardiasis

Inflammatory Bowel Disease (IBD) Treatment
IBD treatment involves minimizing inflammation, controlling symptoms, avoiding flare-ups, and enhancing the patient's quality of life. Treatment approaches differ based on the disease severity, the kind of IBD, and the specific needs of the patient. While there is no cure for IBD, good therapy can result in long periods of remission and better outcomes.
Inflammatory bowel disease (IBD) treatment guidelines include
- Medications
- Surgical treatment for inflammatory bowel disease
- Lifestyle and Dietary Modifications
Medications
Medications are the cornerstone of IBD treatment, and the choice of drugs depends on the disease severity and the patient's response to treatment. In many cases, treatment begins with amino salicylates (5-ASA), which are anti-inflammatory medications. These drugs are primarily used to treat mild to moderate cases of ulcerative colitis. They reduce inflammation in the colon and rectum and are often used for long-term maintenance therapy. However, while amino salicylates are effective for many people with ulcerative colitis, their efficacy in Crohn's disease is more limited.
In patients with moderate to severe inflammation or those experiencing flare-ups, corticosteroids may be prescribed. These drugs are potent anti-inflammatory agents that can quickly reduce inflammation. However, corticosteroids are typically used for short periods due to their significant side effects, such as weight gain, osteoporosis, and increased infection risk. For long-term management, corticosteroids are generally avoided in favor of other medications.
For patients who do not respond to amino salicylates or corticosteroids, immunosuppressive medications may be introduced.
These drugs are often used in combination with other treatments for moderate to severe disease, particularly when corticosteroids alone are ineffective or cause undesirable side effects.
Biologic therapies are a breakthrough in the treatment of IBD, particularly for patients with moderate to severe IBD who have not responded to conventional medications. Tumor necrosis factor (TNF) inhibitors are biologic drugs that block the action of TNF, a protein involved in inflammation. These drugs are more effective in treating both ulcerative colitis and Crohn’s disease, and they can help induce remission and maintain long-term control of the disease.
Other biologic agents include integrin inhibitors, which block the passage of immune cells to the inflammation site in the intestines, and interleukin inhibitors, which target specific cytokines involved in the inflammatory process. Biologic therapies are generally reserved for more severe forms of IBD, particularly when other medications have failed.
Antibiotics are occasionally used in the treatment of IBD, especially when complications like abscesses or infections arise. They may be used for Crohn's disease or when an infection complicates the disease course. However, antibiotics are not considered a primary treatment for IBD and are typically used only when needed.
For patients with diarrhea, which is a common and distressing symptom of IBD, anti-diarrheal medications can help control symptoms. However, these medications are recommended to be used cautiously during active flare-ups because they can cause complications like bowel obstruction.
Surgical treatment for inflammatory bowel disease
In some cases, surgery becomes necessary, either because medications are no longer effective or because the disease has led to complications. Surgery for ulcerative colitis may involve the removal of the colon (colectomy), which effectively cures the disease. A J-pouch procedure may be performed, in which a new reservoir is created from the small intestine to replace the colon, allowing patients to have more normal bowel function.
In Crohn's disease, surgery is generally used to treat complications such as bowel obstructions, abscesses, or fistulas. Unlike ulcerative colitis, however, surgery does not cure Crohn's disease, and the disease often recurs in other parts of the gastrointestinal tract after surgery. Surgical interventions like intestinal resections, in which sections of the intestines are removed, can help manage symptoms and complications, but they do not eliminate the underlying disease.
Lifestyle and Dietary Modifications
While there is no specific "IBD diet," patients with IBD may benefit from dietary modifications, particularly during flare-ups. Certain foods can exacerbate symptoms, so patients often need to avoid high-fat, high-fiber, or dairy products, especially during times of active inflammation. A low-residue diet (diet that reduces the amount of food waste in the large intestine), which limits the intake of fiber, may be recommended to reduce the risk of bowel obstruction during flare-ups.
Patients may also need nutritional support, as malabsorption is common in IBD. Vitamin and mineral supplementation are important for those with chronic disease, particularly for deficiencies in iron, vitamin B12, calcium, and vitamin D.
Since stress can trigger IBS, it is necessary that along with dietary modifications, stress management plays an important role in managing IBD. Mindfulness, relaxation exercises, and regular physical activity are some effective ways that can reduce stress and promote general well-being.
IBD Treatment Cost in Hyderabad, India
The cost of IBD (Inflammatory Bowel Disease) Treatment in Hyderabad generally ranges from ₹1,000 to ₹65,000 (approx. US $12 – US $780).
The exact cost depends on whether the condition is Ulcerative Colitis or Crohn’s Disease, severity of symptoms, requirement for diagnostic tests (blood tests, stool tests, colonoscopy, imaging), medications (5-ASA, steroids, immunomodulators, biologics), hospitalization needs, nutritional therapy, and hospital facilities — including cashless treatment options, TPA corporate tie-ups, and insurance support wherever applicable.
Cost Breakdown According to Type of IBD Treatment
- Gastroenterologist Consultation – ₹800 – ₹1,800 (US $10 – US $22)
- Basic Blood Tests (CBC, CRP, ESR) – ₹600 – ₹1,800 (US $7 – US $22)
- Stool Tests (Calprotectin, Occult Blood) – ₹800 – ₹3,000 (US $10 – US $36)
- Colonoscopy (With Biopsy) – ₹7,000 – ₹16,000 (US $85 – US $190)
- CT / MRI Enterography – ₹8,000 – ₹18,000 (US $95 – US $215)
- Medical Therapy (5-ASA / Steroids) – ₹600 – ₹2,500/month (US $7 – US $30)
- Immunosuppressants (Azathioprine / 6-MP) – ₹300 – ₹1,200/month (US $4 – US $14)
- Biologic Therapy (If Required) – ₹18,000 – ₹65,000/dose (US $215 – US $780)Hospitalization for Severe Flare – ₹12,000 – ₹30,000 (US $145 – US $360)
- Nutritional & Diet Therapy – ₹600 – ₹2,000 (US $7 – US $24)
Frequently Asked Questions (FAQs) on IBD Treatment
What are the first-line treatments for newly diagnosed IBD?
Initial treatments depend on disease severity and location. Mild-to-moderate cases typically begin with anti-inflammatory medications for ulcerative colitis or locally acting steroids for Crohn's disease. Moderate-to-severe cases might require conventional steroids for quick symptom control, followed by immune system modulators or targeted biologic therapies for ongoing management.
Which Is the best hospital for IBD Treatment in Hyderabad, India?
PACE Hospitals, Hyderabad, is one of the most trusted centres for diagnosing and managing Inflammatory Bowel Disease, including Ulcerative Colitis and Crohn’s Disease.
Our team of experienced gastroenterologists offers comprehensive evaluation and targeted treatment for:
- Mild, moderate, and severe Ulcerative Colitis
- Crohn’s Disease involving small bowel or colon
- IBD-related strictures, fistulas, and complications
- Nutritional deficiencies due to chronic inflammation
- Extraintestinal manifestations (joints, skin, liver)
With advanced endoscopy, colonoscopy with biopsy, MRI/CT enterography, specialised IBD clinic protocols, nutritional support, and emergency care for flare-ups, PACE Hospitals ensures accurate diagnosis, effective treatment, and long-term disease control — supported by cashless insurance, TPA tie-ups, and complete documentation assistance.
When is surgery necessary for IBD treatment?
Surgery becomes necessary when medications fail to control symptoms, complications arise (narrowing, abnormal connections, abscesses, perforation), or when cancer develops. For ulcerative colitis, removing the colon can cure the disease. Crohn's disease surgery addresses specific complications but isn't curative, with 70-80% of patients eventually needing additional operations as the disease returns.
What causes inflammatory bowel disease?
The actual cause of inflammatory bowel disease is still not because nothing has been concretely, found out what is the exact pathogenesis of IBD? It has been said that sometimes infection can cause, dietary alterations can cause, alterations in intestinal microbial flora can cause, and sometimes ethnic variations are also there because this is predominantly seen in the Western world compared to the Eastern world. And sometimes genetic tendencies may also be there, because it is some little common in some specific antigens, so it's multifactorial.
What dietary changes can help manage IBD symptoms?
Dietary management varies by person but often includes identifying trigger foods through elimination diets or food journals. Special diets that limit certain carbohydrates or focus on anti-inflammatory foods show promise for symptom reduction. Adequate protein, calorie, and nutrient intake prevents malnutrition. During flares, low-fiber or liquid nutrition may rest the bowel while maintaining nourishment.
What Is the cost of IBD Treatment at PACE Hospitals, Hyderabad?
At PACE Hospitals, Hyderabad, the cost of IBD treatment typically ranges from ₹900 to ₹52,000 and above (approx. US $11 – US $625), making it an affordable and specialised option for patients with Ulcerative Colitis or Crohn’s Disease. However, the final cost depends on:
- Type of IBD (Ulcerative Colitis vs. Crohn’s Disease)
- Severity and frequency of flare-ups
- Requirement for colonoscopy, imaging, and biopsy
- Medication type (5-ASA, steroids, immunosuppressants, biologics)
- Need for hospitalization during severe inflammation
- Nutritional therapy and lifestyle counselling
- Associated complications (strictures, bleeding, fistulas)
- Long-term monitoring and follow-up visits
Patients with mild disease requiring routine medication fall at the lower end, while those requiring biologics, advanced imaging, or hospitalization fall towards the higher range.
After gastroenterology evaluation, necessary tests, and disease assessment, our specialists will provide a personalized treatment plan and a transparent cost estimate based on your clinical needs.
What are the latest treatment advances for IBD?
Recent advances include new oral medications that work differently from injectable biologics, and substances affecting immune cell movement. Increasingly targeted biologics focus on specific inflammatory pathways. Emerging approaches include gut-selective therapies, optimized combination treatments, and interventions targeting the gut microbiome (bacterial community).
How to cure / treat inflammatory bowel disease permanently?
This is very difficult because curing inflammatory bowel disease is challenging, and one has to accept the condition that it is controllable but not curable. Just like a person suffering from diabetes, support and suffering from hypertension, they have to be on lifelong medication, lifelong checkups, blood sugar monitoring. Same with inflammatory bowel disease (IBD), it should be constantly monitored and see for any red flag signs. If the patient is having fever or acute abdomen pain or a lot of blood loss in the motion, they have to consult the doctor immediately. Otherwise, they have to be regularly maintained and frequent checkups.
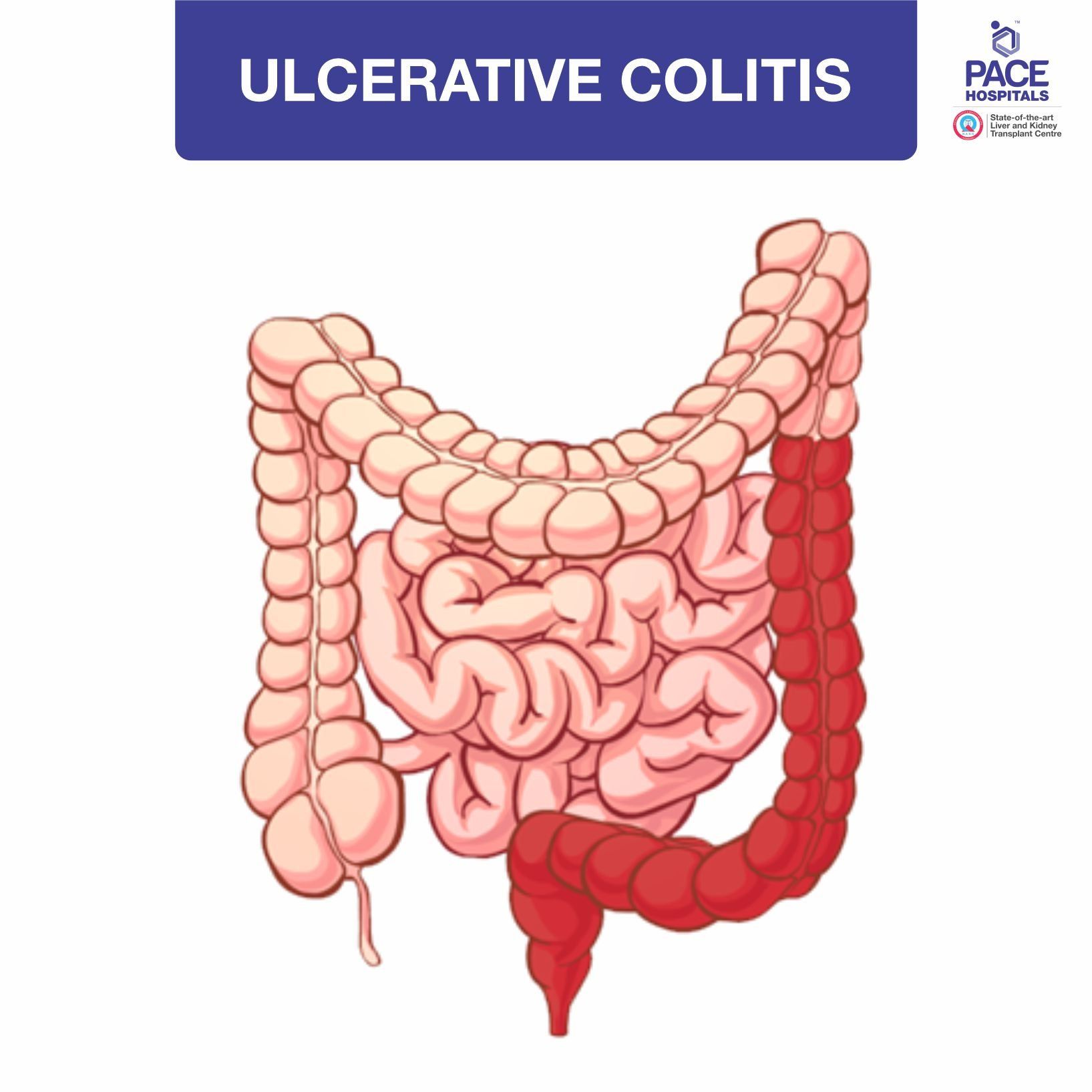
What is inflammatory bowel disease (Ulcerative colitis and Crohn's disease)?
Inflammatory bowel disease bowel disease encompasses two major components, Ulcerative colitis and Crohn's disease. Ulcerative colitis as the term indicates, predominantly involves the colon and less of the small intestine, whereas Crohn's disease predominantly affects the small intestine but you can also involve the large intestine. How do you differentiate? Differentiation is mainly by doing the colonoscopy examination, by taking the history and also imaging studies.
What are the types of inflammatory bowel disease (IBD)?
There are mainly two types of inflammatory bowel disease (IBD): Crohn's disease and ulcerative colitis.
- Crohn’s disease affects any part of the digestive system, most commonly the small intestine and the beginning of the large intestine, causing patchy, deep inflammation that may lead to pain, diarrhea, tiredness, and weight loss.
- Ulcerative colitis only affects the large intestine and rectum, causing continuous inflammation, ulcers, and bleeding, which often result in bloody diarrhea and abdominal cramps.
What tests are used to diagnose inflammatory bowel disease?
Gastroenterologists use several tests including blood tests to check for inflammation, stool samples to rule out infections, and camera procedures like colonoscopy with tissue samples. Special imaging like MRI or CT scans of the digestive tract helps visualize the bowels. A swallowable camera may examine areas where standard scopes can't reach in suspected cases.
What is the difference between crohn's disease and ulcerative colitis?
Ulcerated colitis predominantly affects the colon, whereas the Crohn's disease, predominantly the small intestine and presentation wise, we cannot differentiate how the patient presents, but if the patient presents with vomiting and signs of obstruction intestinal obstruction, we suspect Crohn's. And the patient having a lot of blood in mucus in the stool, we suspect Ulcerated colitis. However, the main diagnostic mode is colonoscopy.
How do doctors differentiate between Crohn's disease and ulcerative colitis?
Gastroenterologists tell these IBD types apart through camera examinations - Crohn's disease shows patchy inflammation that can appear anywhere from the mouth to the anus with healthy areas in between. Ulcerative colitis shows continuous inflammation only in the colon/rectum affecting just the inner lining. Tissue samples under microscopes reveal different patterns in each condition.
How long does ulcerative colitis last?
Ulcerative colitis is a condition which is sometimes can be self-limiting. Sometimes it can go with relapses and this relapses can be a long-standing one, because depending on the main cause of the ulcerative colitis, if we don't attend to the causes this control on and can lead to a pan colitis and recurrent symptoms were almost years together. So in such a case, will have to be tackled very appropriately and at the right time. So to prevent any further relapse and extension of the colitis.
What is the best treatment for ulcerative colitis?
This is really sort of difficult to answer because there are so many modes of treating ulcerative colitis, starting for basic medications and through high-level immunomodulators sometimes we have to do total colectomy. So depending on the case will have to decide what appropriate treatment is required. This is adjusted by knowing, the severity of the ulcerative colitis. Depending on the involvement where there's only sigmoid, colon, rectum is involved, or the descending colon is involved or transverse or sometimes ascending colon. So depending on the site of involvement again, the appropriate therapy is advised and further depends upon the amount of blood loss upon the CRP level of the toxicity levels. Systemic symptoms like fever, tachycardia. In this will have to give some steroids also. So it depends on the type of patient which treatment suits to which patient. It will be customized according to symptoms and severity.
What is a stricture in crohn's disease?
Crohn's disease predominant involves a small intestine, so a long-standing Crohn's disease can lead to fibrosis of the intestines at intermittently levels, and this can lead to sometimes a partial obstruction or a total obstruction. This narrowing of the small intestine is known as a stricture. This presents predominantly with the stomach pain and then repeated vomiting. The treatment for this stricture, once it occurs medically, cannot be corrected. But sometimes patients may have to undergo surgery if the stitches are accessible. We can do dilatation or stent placement.
What is the most effective treatment for crohn's disease?
It depends the severity of the Crohn's disease. A mild case of Crohn's can be tackled with medical therapy, improving the immunity of the person. But if any patient comes with severe strictures and obstruction, the best modes only intersection and bypassing the structure.
What symptoms should someone prompt to get tested for IBD?
Ongoing diarrhea for more than six weeks, blood in the stool, unexplained weight loss, constant tiredness, stomach cramps, symptoms that wake-up individuals at night, and a family history of IBD warrant a gastroenterologist visit. Problems outside the gut like joint pain, eye inflammation, skin rashes, or mouth sores alongside digestive issues particularly suggest possible IBD.
Is a colonoscopy always necessary for IBD diagnosis?
While colonoscopy remains the best method for IBD diagnosis by allowing direct viewing and tissue sampling, alternatives exist for certain patients. Children or those unable to undergo this procedure might start with less invasive imaging tests. However, a definitive diagnosis typically requires examination with a scope and tissue confirmation.
What biomarkers are used in IBD diagnosis?
Key indicators include stool tests that measure gut inflammation without invasive procedures. Blood tests check general inflammation signals, complete blood count, and protein levels. Newer blood tests look for specific antibodies that often appear with Crohn's disease or ulcerative colitis, helping distinguish between these conditions.
How accurate are stool tests in diagnosing IBD?
Stool tests measuring inflammation markers are about 85-90% reliable in detecting intestinal inflammation, making them excellent screening tools. However, they can't definitively diagnose IBD or tell which type that a patient has. These tests work well for tracking disease activity and predicting flare-ups while reducing unnecessary invasive procedures.
What role does imaging play in IBD diagnosis (MRI, CT, ultrasound)?
Imaging techniques show the intestinal walls and surrounding tissues, particularly helpful for Crohn's disease. MRI provides detailed images without radiation exposure. CT scans offer quick assessment during urgent situations. Ultrasound allows real-time evaluation of bowel wall thickness and blood flow, especially valuable for children.
Are there genetic tests for IBD?
While genetic testing isn't routinely used for diagnosis, tests detecting IBD-related gene variations exist. These tests mainly help assess risk and understand disease mechanisms rather than confirming a diagnosis. Family members with certain genetic markers might benefit from earlier screening, though environmental factors remain equally important in developing IBD.
How are IBD flares distinguished from other digestive conditions?
Distinguishing IBD flares involves evaluating symptom patterns, inflammation markers and stool tests to rule out infections, and often camera examinations. Key differences include duration (IBD symptoms typically last weeks), problems outside the digestive system, nighttime symptoms, and how symptoms respond to previous IBD treatments versus temporary relief from anti-diarrhea medications.
What is the diagnostic process for pediatric IBD?
Childhood IBD diagnosis combines growth chart review, family history, lab tests (including stool inflammation markers), and examination of the upper and lower digestive tract with tissue samples. Special classification systems categorize disease subtypes. Imaging uses techniques that limit radiation when possible. Psychological assessment is essential, addressing unique challenges of childhood onset.
How do biologics work for treating IBD?
Biologic medications target specific inflammation-causing proteins that drive IBD. Anti-inflammatory biologics neutralizes substances that cause inflammation. Gut-specific biologics block inflammatory cells from entering the intestine. Other biologics inhibit specific inflammatory pathways. These targeted treatments reduce inflammation more precisely than traditional medications, potentially offering better long-term control with fewer whole-body side effects.
What are the differences between immunomodulators and biologics?
Immunomodulators broadly suppress immune function, work gradually over weeks/months and are taken orally or by injection. Biologics target specific inflammatory pathways using engineered proteins, work faster, require intravenous or under-the-skin administration, and often work better for moderate-to-severe disease while offering more precise immune regulation.
How are IBD flares treated differently from maintenance therapy?
Flare treatment focuses on quick symptom control using steroids, increased biologic dosing, or additional topical treatments. Maintenance therapy aims for long-term remission through immune-modifying medications or anti-inflammatories at regular intervals. Flare management may require hospitalization, bowel rest, or IV medications, while maintenance emphasizes sticking with treatment, monitoring, and preventing complications.
How are treatment plans personalized for different IBD patients?
Treatment personalization considers disease type (Including location, behavior, severity), previous treatment response, other health conditions, and increasingly, biological markers and genetic factors. Patient preferences regarding how medicine is given, lifestyle impacts, and pregnancy plans influence decisions. The "treat-to-target" approach uses objective markers alongside symptom control to guide therapy adjustments.
What are the potential side effects of common IBD medications?
Anti-inflammatory medications may cause headaches or stomach discomfort. Steroids risk mood changes, bone loss, and metabolic effects. Immune system modulators can affect bone marrow, liver, or pancreas. Biologics increase infection risk and may cause reactions during administration. All immune-suppressing therapies require monitoring for a potentially increased cancer risk.
What complementary or alternative treatments show promise for IBD?
Emerging complementary approaches include medical cannabis compounds, acupuncture, mind-body techniques, turmeric supplements, and specialized beneficial bacteria. Omega-3 fatty acids show modest anti-inflammatory effects. Peppermint oil preparations may reduce IBS-like symptoms in IBD. These approaches typically complement rather than replace conventional treatments, ideally used with medical supervision.
How is treatment monitored for effectiveness?
Monitoring combines symptom assessment, inflammation markers, endoscopic examinations, and imaging. Medication level testing measures drug concentration and antibodies to optimize dosing. Patient-reported questionnaires track quality of life impacts. Regular laboratory work screens for medication effects on liver, kidneys, and blood counts.
What treatment options exist for IBD patients who don't respond to conventional therapies?
Options for hard-to-treat IBD include switching medication classes (trying different biologics targeting alternate pathways), combination therapy using biologics with immune modulators, experimental treatments through clinical trials, surgical options for suitable candidates, intensive nutritional support, and specialized centers offering stem cell treatments for carefully selected cases with severe treatment-resistant disease.
How do treatment approaches differ between Crohn's disease and ulcerative colitis?
Ulcerative colitis primarily responds to anti-inflammatory medications, whereas they show limited benefit in Crohn's. Certain biologics work faster in ulcerative colitis. Surgical approaches differ fundamentally – colon removal potentially cures ulcerative colitis while Crohn's surgery addresses specific complications. Ulcerative colitis treatment follows a more standardized approach, while Crohn's often employs more aggressive early strategies for high-risk cases.
What role do probiotics play in IBD treatment?
Specific beneficial bacteria formulations show modest benefits in ulcerative colitis and inflammation after surgery, particularly certain well-studied strains. Evidence remains limited for Crohn's disease. Probiotics may help maintain remission, reduce inflammation, and restore bacterial balance. Their role represents additional therapy rather than primary treatment, with specific strains showing benefits rather than all probiotics.
How are steroids used in IBD treatment and what are their limitations?
Steroids quickly control inflammation during moderate-to-severe flares but aren't suitable for long-term use due to significant side effects. They're typically reduced gradually over weeks once symptoms improve. Limitations include bone loss, metabolic problems, mood changes, infection risk, and adrenal gland suppression. Newer-generation steroids offer more targeted action with fewer whole-body effects.
Why PACE Hospitals, regarded as the first choice for Inflammatory Bowel Disease (IBD) Treatment in Hyderabad, India?
PACE Hospitals is well known as the best hospital for Inflammatory Bowel Disease (IBD) Treatment in Hyderabad, India, providing expert care for patients with chronic digestive inflammation. Our skilled gastro doctor in Hyderabad specialize in accurate inflammatory bowel disease diagnosis and perform advanced IBD tests to determine the severity and type of IBD disease, including Crohn’s disease and ulcerative colitis. We focus on personalized inflammatory bowel disease treatment and long-term management of inflammatory bowel disease through medication, dietary guidance, and lifestyle modifications. With evidence-based therapies, continuous monitoring, and patient-centered care, PACE Hospitals ensures effective and lasting IBD treatment for improved digestive health and quality of life.




