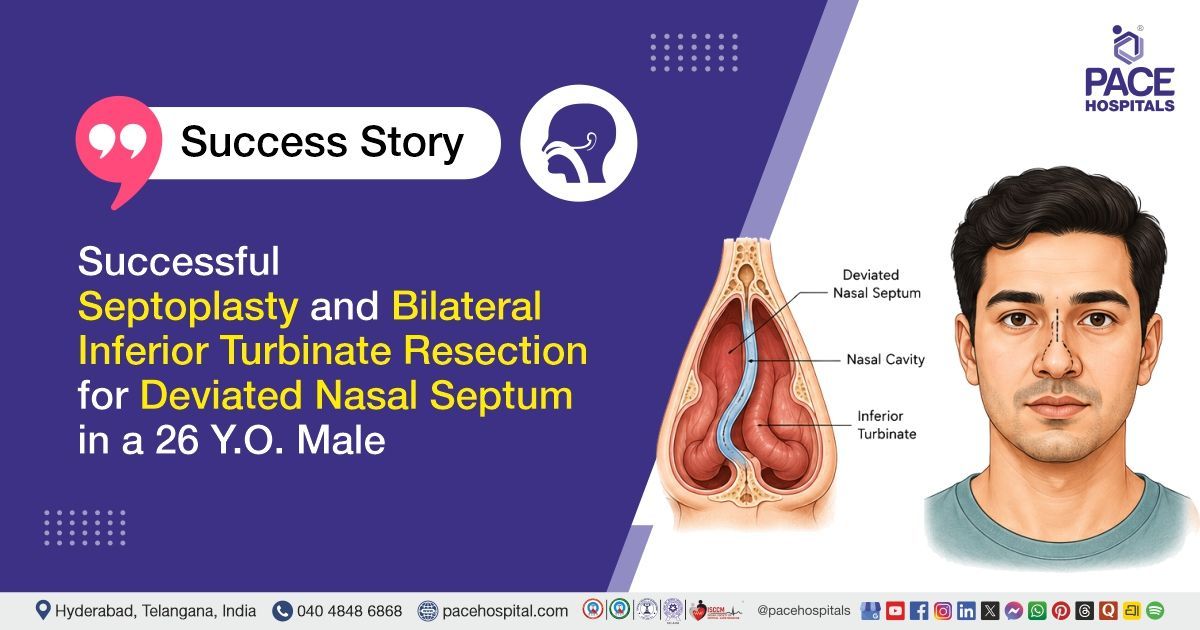
Successful Septoplasty & Bilateral Inferior Turbinate Resection for Deviated Nasal Septum
PACE Hospitals
PACE Hospital’s expert ENT team successfully performed a Septoplasty with Bilateral Inferior Turbinate Submucosal Resection (Turbinectomy) on a 26-year-old male patient diagnosed with Deviated Nasal Septum (DNS) and Bilateral Inferior Turbinate Hypertrophy. The procedure was undertaken to correct the nasal septal deviation and reduce the enlarged inferior turbinates, with the aim of improving nasal airflow, relieving chronic nasal obstruction, enhancing breathing comfort, and improving the patient’s overall quality of life.
Chief Complaints
A 26-year-old male patient with a Body Mass Index (BMI) of 20 presented to the ENT Department at PACE Hospitals, Hitech City, Hyderabad, with complaints of bilateral nasal obstruction, more pronounced on the left side, for the past six months. The symptoms began following a nasal injury sustained from a cricket ball six months earlier, which was associated with an episode of nasal bleeding. The patient denied any history of nasal discharge, excessive sneezing, recurrent headaches, ear pain, or other associated ENT complaints.
Past Medical History
The patient had no significant past medical history and was not known to have any chronic illnesses such as hypertension, diabetes mellitus, bronchial asthma, or cardiovascular disease. There was no history of previous surgeries, hospitalizations, or long-term medication use. The patient also had no known drug or food allergies and was otherwise in good general health prior to presentation.
On Examination
On examination, the patient was conscious, coherent, and well-oriented to time, place, and person, with no apparent distress. Nasal examination revealed a left-sided deviated nasal septum and bilateral inferior turbinate hypertrophy, resulting in nasal obstruction. There was no tenderness over the paranasal sinuses. Bilateral tympanic membranes were intact, and the oral cavity examination was normal. No significant abnormalities were detected on the remainder of the systemic examination.
Diagnosis
After the initial examination, the patient underwent a comprehensive evaluation by the ENT team, which included a detailed clinical assessment, anterior rhinoscopic examination, nasal endoscopic evaluation, and radiological assessment with a CT scan of the paranasal sinuses. These investigations were performed to determine the cause of his persistent nasal obstruction and assess the extent of structural abnormalities affecting nasal airflow.
Clinical examination revealed a significant deviation of the nasal septum toward the left side along with bilateral inferior turbinate hypertrophy. The paranasal sinuses were non-tender on examination, and bilateral tympanic membranes were intact. Oral cavity examination was unremarkable. CT imaging further confirmed a high left-sided deviated nasal septum and bilateral inferior turbinate hypertrophy, correlating with the patient's symptoms of chronic nasal blockage.
Following a thorough evaluation and correlation of the clinical and radiological findings, the patient was diagnosed with Deviated Nasal Septum (DNS) with Bilateral Inferior Turbinate Hypertrophy. The septal deviation, likely exacerbated by the history of nasal trauma, along with turbinate enlargement, was identified as the primary cause of the patient's persistent nasal obstruction and impaired nasal airflow.
Based on comprehensive evaluation, the patient was advised to undergo Deviated Nasal Septum with Bilateral Inferior Turbinate Hypertrophy Treatment in Hyderabad, India, under the ENT Department to correct the septal deviation, reduce turbinate hypertrophy, restore nasal airflow, and relieve nasal obstruction, thereby improving breathing and overall quality of life.
Medical Decision Making
After a thorough consultation with Dr Mohana Jambula (ENT Surgeon), a comprehensive evaluation was carried out to determine the most appropriate diagnostic and therapeutic approach for the patient. The assessment focused on identifying the underlying cause of persistent nasal obstruction, with clinical and radiological correlation confirming a deviated nasal septum with bilateral inferior turbinate hypertrophy.
Based on the clinical findings, CT scan reports, and systemic examination, it was determined that Septoplasty with Bilateral Inferior Turbinate Submucosal Resection under general anaesthesia was the most appropriate and definitive treatment. The procedure was planned to correct the septal deviation, reduce turbinate hypertrophy, restore normal nasal airflow, and relieve chronic nasal obstruction.
The patient and his family were thoroughly counselled regarding the diagnosis, indication for surgery, expected benefits, and possible risks associated with the procedure. The primary aim of management was to achieve symptomatic relief, improve nasal breathing, and enhance overall quality of life.
Surgical Procedure
Following the diagnosis, the patient was scheduled to undergo Bilateral Inferior Turbinate Submucosal Resection with Septoplasty Surgery in Hyderabad at PACE Hospitals, under the expert care of the ENT Department.
The procedure was performed in the following steps:
- Patient Positioning and Preparation: The patient was placed in the reverse Trendelenburg position under general anaesthesia. The nasal and surrounding facial areas were painted and draped under strict aseptic precautions to maintain a sterile surgical field.
- Nasal Decongestion and Local Preparation: Bilateral nasal cavities were decongested. Local infiltration of 2% local anesthetic with catecholamine was administered, followed by packing with 4% local anesthetic to achieve adequate mucosal anaesthesia and vasoconstriction, thereby minimizing intraoperative bleeding.
- Septal Correction (Septoplasty): A left Killian incision was made, and endoscopic septoplasty was performed. The deviated nasal septum was corrected, and the septum was realigned to improve nasal airflow and structural alignment.
- Mucosal Flap Repositioning and Turbinate Reduction: Bilateral mucoperichondrial and mucoperiosteal flaps were carefully repositioned and secured using Vicryl sutures. This was followed by bilateral inferior turbinate submucosal resection to reduce turbinate hypertrophy and further improve nasal patency.
- Hemostasis and Nasal Packing: Complete haemostasis was achieved throughout the procedure. Both nasal cavities were packed with Ivalon nasal packs (1+1), and appropriate dressing was applied. The immediate postoperative period was uneventful with stable intraoperative findings.
Postoperative Care
The immediate postoperative period was uneventful, and the patient remained hemodynamically stable. Postoperatively, the patient was managed with medications to prevent postoperative infection, reduce gastric acidity to prevent stress-related gastric irritation, and provide relief from postoperative pain. Nasal care was maintained with appropriate local management, and nasal packs were removed as per standard protocol. The patient demonstrated satisfactory recovery and was monitored closely in the postoperative period.
Discharge Medications
Upon discharge, the patient was prescribed medications for prevention of postoperative infection, reduction of gastric acidity and related discomfort, relief of postoperative pain, control of allergic symptoms, and reduction of nasal inflammation to promote healing and improve nasal breathing following surgery. These were advised for a specified duration as part of routine postoperative care after septoplasty with bilateral inferior turbinate submucosal resection.
Advice on Discharge
The patient was advised to avoid forceful nose blowing and to refrain from lifting heavy weights to prevent postoperative complications and ensure proper healing.
Emergency Care
The patient was informed to contact the emergency ward at PACE Hospitals in case of any emergency or development of symptoms such as fever, nasal bleeding, or vomiting.
Review and Follow-up Notes
The patient was advised to follow up with the ENT specialist in Hyderabad at PACE Hospitals for further evaluation of the surgical site and overall progress.
Conclusion
This case highlights successful surgical management of a deviated nasal septum with bilateral inferior turbinate hypertrophy using septoplasty and bilateral inferior turbinate submucosal resection. The procedure was completed without complications and the postoperative period was uneventful. The patient showed good recovery with improvement in nasal airflow and was discharged in stable condition with a satisfactory outcome.
Surgical Management of Deviated Nasal Septum with Inferior Turbinate Hypertrophy
Deviated nasal septum with inferior turbinate hypertrophy is a common anatomical cause of chronic nasal obstruction. Patients typically present with persistent nasal blockage, mouth breathing, and reduced quality of life when conservative management fails. Accurate clinical evaluation, along with endoscopic and radiological assessment, is essential for confirming the diagnosis and planning appropriate intervention. Septoplasty with inferior turbinate reduction is the definitive surgical treatment aimed at restoring normal nasal anatomy and improving airway patency.
The procedure is generally safe and effective when performed under proper aseptic precautions and surgical expertise by an Otolaryngologist / ENT specialist. Postoperative outcomes are usually favorable, with significant improvement in nasal airflow and symptom relief. Early recognition and timely surgical correction help prevent long-term complications and improve overall patient well-being.
Frequently Asked Questions (FAQs)
How long does recovery take after septoplasty with inferior turbinate reduction?
Recovery after septoplasty with turbinate reduction is usually quick. Most people feel much better within 1 to 2 weeks. Some nasal blockage, swelling, crusting, and mild discomfort are common during the first few days. Breathing improves gradually as the swelling settles. The inside of the nose may take several weeks to heal completely.
Why is turbinate reduction done along with septoplasty?
Septoplasty is a surgical procedure used to correct a deviated nasal septum and improve airflow through the nose. Turbinate reduction is done to reduce the size of enlarged turbinates that can also cause nasal blockage. When both problems are present, treating only the deviated septum may not completely relieve the obstruction. In such cases, treating both the septum and turbinates together usually gives better improvement in nasal breathing.
When can a patient breathe normally after nasal pack removal?
Many patients notice some improvement in breathing once the nasal packs are removed. However, the nose may still feel blocked because of swelling and crusting inside the nasal passages. This usually improves over the next several days. Following the doctor's instructions and avoiding forceful nose blowing can help recovery.
Is septoplasty useful for nasal blockage after nasal injury?
Yes. Injury to the nose can sometimes cause or worsen a deviated nasal septum, which means the wall between the two sides of the nose becomes crooked. This can lead to long-term nasal blockage and difficulty in breathing through the nose.
Septoplasty is a surgical procedure used to straighten this deviated septum and improve airflow through the nasal passages. It is usually recommended when symptoms such as nasal blockage continue even after medical treatment.
Can a deviated nasal septum return after septoplasty?
Septoplasty generally provides lasting correction of a deviated septum. In some cases, healing changes, a small remaining deviation, or a future injury to the nose may affect the final result. Following post-operative instructions and attending follow-up visits can help ensure proper healing.
What precautions should be followed after septoplasty and turbinate surgery?
During recovery, patients should avoid lifting heavy objects, doing hard physical exercise, forcefully blowing the nose, or any activity that may injure the nose. Resting with the head slightly raised can help reduce swelling. All nasal care instructions given by the ENT specialist should be followed carefully. If there is any unusual bleeding, fever, or severe pain, it should be reported to the doctor immediately.
Is nasal packing always required after septoplasty?
Nasal packing is not needed in all cases. It is used depending on the type of surgery and the patient’s condition. When placed, it helps control bleeding and supports healing inside the nose. It is usually removed a short time after surgery. While it is in place, patients may feel mild discomfort and a blocked feeling in the nose, which is normal.
Can septoplasty and turbinate reduction improve sleep quality?
Yes, these procedures can help improve sleep in people whose sleep issues are due to nasal blockage. When breathing through the nose becomes easier, it can reduce mouth breathing and make sleep more comfortable. However, problems like snoring or sleep apnea may need further evaluation and additional treatment.
What are the possible risks after septoplasty with turbinate reduction?
Like any surgical procedure, septoplasty and turbinate reduction have some risks. In the short term, patients may notice mild bleeding, swelling, crusting inside the nose, discomfort, and a blocked sensation in the nose. In rare cases, problems such as infection, a small hole in the nasal septum, changes in smell, or persistent nasal blockage may occur. Most patients recover well without any major complications.
When can normal activities be resumed after septoplasty?
Most patients are able to return to light daily activities within a few days after surgery. However, strenuous activities such as heavy exercise, weight lifting, frequent bending, or contact sports should be avoided until proper healing has taken place. The ENT specialist will guide the patient on when it is safe to resume normal and full physical activities depending on the recovery progress.
Share on
Request an appointment
Fill in the appointment form or call us instantly to book a confirmed appointment with our super specialist at 04048486868
Appointment request - health articles
Recent Articles