Successful C3–C5 Cervical Stabilization & C3–C4 Laminectomy for Cervical Canal Stenosis
PACE Hospitals
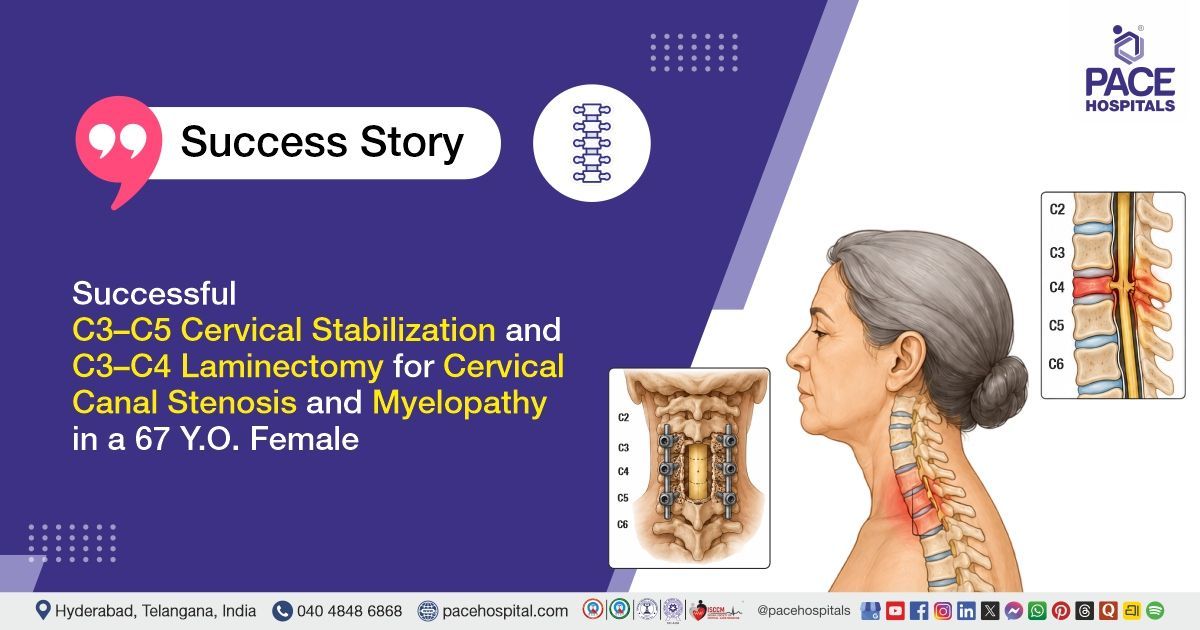
PACE Hospitals' expert Neurosurgery team successfully performed a C3–C5 Posterior Cervical Stabilization with Posterolateral Fusion and C3–C4 Laminectomy on a 67-year-old female patient diagnosed with C3–C4 intervertebral disc prolapse (IVDP) with cervical canal stenosis and cervical myelopathy. The procedure was performed to relieve spinal cord compression and stabilize the cervical spine. It aimed to prevent further neurological deterioration and improve the patient's limb strength and mobility.
Chief Complaints
A 67-year-old female patient with a body mass index (BMI) of 21 presented to the Neurosurgery Department at PACE Hospitals, Hitech City, Hyderabad, with a two-week history of gradually progressive weakness in all four limbs, more pronounced on the right side. She also reported chronic neck pain and low backache, for which she had been taking over-the-counter medications. There was no history of trauma or urinary or bowel incontinence.
Past Medical History
She was a known hypertensive and was on regular treatment. There was no history of trauma, prior cervical spine surgery, or bowel and bladder dysfunction before presentation.
On Examination
On examination, the patient was moderately built and nourished, with stable vital signs. Neurological examination revealed weakness in all four limbs, more pronounced on the right side, along with increased muscle tone, exaggerated deep tendon reflexes, and bilateral extensor plantar responses, suggestive of cervical myelopathy. Cranial nerve examination was normal, cerebellar signs were absent, and there were no signs of meningeal irritation. Cardiovascular, respiratory, and abdominal examinations were normal.
Diagnosis
Upon admission to PACE Hospitals, the patient underwent a comprehensive clinical evaluation along with a detailed review of her medical history and neurological examination by the Neurosurgery team.
Laboratory investigations revealed mild microcytic hypochromic anemia with neutrophilic predominance, while renal function tests and serum electrolyte levels were within normal limits. Clinical examination demonstrated weakness in all four limbs, more pronounced on the right side, increased muscle tone, exaggerated deep tendon reflexes, and bilateral extensor plantar responses, consistent with cervical myelopathy.
Radiological evaluation of the cervical spine confirmed C3–C4 intervertebral disc prolapse (IVDP) with cervical canal stenosis and spinal cord compression (cervical myelopathy). The imaging findings correlated with the patient's progressive quadriparesis and chronic neck pain, necessitating surgical intervention.
Based on the confirmed diagnosis, the patient was advised to undergo C3-C4 IVDP with Cervical Canal Stenosis and Myelopathy Treatment in Hyderabad, India, under the expert care of the Neurosurgery Department to decompress the spinal cord and stabilize the cervical spine.
Medical Decision-Making (MDM)
After a detailed clinical evaluation by Dr. U. L. Sandeep Varma (Consultant Neurosurgeon), the patient presented with progressive weakness of all four limbs, more pronounced on the right side, associated with signs of cervical myelopathy.
Clinical examination and preoperative laboratory investigations, including complete blood picture, renal function tests, and serum electrolytes, were reviewed. Hematological findings revealed mild microcytic hypochromic anemia with neutrophilic predominance, while biochemical parameters were within normal limits. No significant cardiopulmonary contraindications were identified for surgical intervention.
Radiological assessment confirmed C3–C4 intervertebral disc prolapse with cervical canal stenosis and resultant spinal cord compression consistent with cervical myelopathy.
It was determined that C3–C5 posterior cervical stabilization with posterolateral fusion and C3–C4 laminectomy under general anesthesia was the most appropriate surgical approach to decompress the spinal cord, stabilize the cervical spine, prevent further neurological deterioration, and improve functional recovery.
The patient and family were counseled regarding the diagnosis, surgical procedure, postoperative rehabilitation,
physiotherapy, medication adherence, and the importance of regular follow-up for optimal neurological recovery.
Surgical Procedure
Following the decision, the patient was scheduled to undergo a C3–C5 posterior cervical stabilization with posterolateral fusion and C3–C4 laminectomy Surgery in Hyderabad at PACE Hospitals under the expert supervision of the Neurosurgery Department.
The procedure involved the following steps:
- Patient Positioning and Exposure: The patient was placed in the prone position under general anesthesia. The surgical field was prepared and draped under strict aseptic precautions, and a vertical midline incision was made over the posterior cervical spine. The paraspinal muscles were carefully dissected and separated to expose the underlying vertebral structures.
- Exposure of Cervical Spine Levels: The posterior elements of the cervical spine from C3 to C5 were exposed, including the lamina and lateral masses. Adequate visualization of the operative levels was achieved to facilitate decompression and instrumentation.
- Decompression Procedure: A C3 and C4 laminectomy was performed to decompress the spinal canal and relieve pressure on the spinal cord. Adequate decompression was confirmed intraoperatively, with visible dural pulsations indicating effective spinal cord decompression.
- Instrumentation and Stabilization: Posterior cervical stabilization was achieved by placing lateral mass screws from C3 to C5 with rod fixation. This provided rigid stabilization of the cervical spine following decompression.
- Fusion and Wound Closure: Posterolateral fusion was performed using autologous bone graft to promote long-term spinal stability. Hemostasis was secured, and the surgical wound was closed in layers over a drain. Implants used included lateral mass screws, rods, and connectors.
Postoperative Care
Postoperatively, the patient was shifted to the Intensive Care Unit (ICU) for overnight observation for close neurological and hemodynamic monitoring. She remained stable, and no immediate complications were noted. The surgical drain and urinary catheter were removed on postoperative day two following satisfactory recovery. Early mobilization was initiated, and the patient was encouraged to ambulate with support. The report showed multilevel degenerative changes in the lumbar spine, with severe spinal canal stenosis at L3–L4 due to disc extrusion and nerve compression, and mild to moderate stenosis at other levels with facet joint arthropathy. She was planned for discharge to continue medications as per clinical indications and regular physiotherapy for cervical spine rehabilitation and functional recovery, along with scheduled follow-up for monitoring progress.
Discharge Medications
Upon discharge, the patient was prescribed medications for short-term prevention of postoperative infection, control of neuropathic symptoms, management of postoperative pain and muscle spasm, gastric protection, and support for nerve healing and recovery. She was also continued on long-term therapy for blood pressure control as per her existing medical condition. These medications were advised in appropriate doses and duration as part of postoperative care following cervical spine decompression and stabilization surgery.
Advice on Discharge
The patient was advised that she may take a bath and gradually resume routine activities such as walking and climbing stairs as tolerated. She was instructed to avoid strenuous physical activities and heavy lifting during the recovery period. Regular physiotherapy was recommended as per the rehabilitation protocol to improve neck strength, mobility, and functional recovery following cervical spine surgery.
Emergency Care
The patient was instructed to contact the emergency ward at PACE Hospitals in case of any emergency or development of symptoms, such as fever, worsening weakness in the upper or lower limbs, discharge from the surgical wound, severe neck pain, difficulty in walking, or any new neurological symptoms such as numbness or loss of coordination.
Review and Follow-Up Notes
The patient was advised to return for follow-up with the Neurosurgeon in Hyderabad at PACE Hospitals after 10 days for postoperative review. Staple removal was advised after 8 days, based on wound healing and clinical assessment.
Conclusion
This case highlights cervical myelopathy due to C3–C4 intervertebral disc prolapse with cervical canal stenosis, presenting as progressive quadriparesis. The condition was managed with C3–C5 posterior cervical stabilization, C3–C4 laminectomy, and posterolateral fusion to achieve spinal cord decompression and stability. The postoperative course was stable, and the patient was discharged with planned rehabilitation and follow-up care.
Key Clinical Insight in Cervical Myelopathy Management
Cervical myelopathy is a progressive spinal cord disorder most commonly caused by degenerative changes leading to disc prolapse and cervical canal stenosis. Early identification of upper motor neuron signs such as limb weakness, hyperreflexia, and gait imbalance is essential to prevent irreversible neurological deficits. Surgical decompression, as planned and executed by a neurosurgeon/neurosurgery doctor, remains the definitive treatment in moderate to severe cases to relieve spinal cord compression and halt disease progression.
In cases requiring multilevel decompression, spinal stabilization may be necessary to maintain alignment and prevent postoperative instability. Recovery is often gradual and depends on the duration and severity of preoperative cord compression. Structured rehabilitation and physiotherapy are critical components of postoperative care to enhance functional recovery. Timely intervention by a neurosurgery doctor significantly improves long-term neurological outcomes and quality of life.
Frequently Asked Questions (FAQs)
Why was surgery needed for cervical canal stenosis with myelopathy?
Surgery is usually needed when pressure on the spinal cord causes weakness, walking difficulty, or reduced hand and leg control. Medicines and physiotherapy may reduce pain, but they cannot remove tight compression on the spinal cord. The main aim of surgery is to release the pressure, protect the nerves, and prevent further worsening.
What is C3-C5 cervical stabilization with laminectomy and fusion?
In this surgery, the surgeon removes part of the bone from the back of the neck to create space for the spinal cord. Screws and rods are used to support the affected neck bones from C3 to C5. Bone graft is also placed to help the bones join together and give long-term stability.
How long does recovery take after cervical spine stabilization surgery?
Hospital stay is generally about 3 to 5 days, based on the patient’s recovery. Most patients are able to begin slow walking within 1 to 2 days after surgery. Complete recovery, including improvement in muscle strength and nerve function, usually takes several weeks to months with proper follow-up care and physiotherapy.
Will arm and leg weakness improve after cervical myelopathy surgery?
Weakness may improve gradually after surgery, but the speed of recovery differs from person to person. It depends on how much the spinal cord was compressed and how long the weakness was present before surgery. The surgery mainly stops further damage, while strength improves slowly with healing and physiotherapy.
Is physiotherapy needed after cervical spine surgery?
Yes, physiotherapy is very important after cervical spine surgery. It helps improve walking, balance, muscle strength, and daily movement. Patients should follow the physiotherapy plan advised by the surgeon and avoid doing exercises on their own without guidance.
Can I walk and climb stairs after cervical spine surgery?
Most patients can walk after surgery once the doctor allows it. Stair climbing is also usually possible when the patient is steady and has enough strength. It should be done slowly, with support if needed, and without rushing.
Do screws and rods need to be removed after cervical fusion surgery?
In most cases, screws and rods are kept permanently inside the neck. They are placed to support the spine while the bones fuse and heal. Removal is usually not needed unless there is pain, infection, loosening, or another implant-related problem.
What should be avoided after cervical spine fusion surgery?
Patients should avoid lifting heavy objects and making sudden movements of the neck. They should also not bend or twist the neck forcefully or do strenuous physical work or high-impact exercises. These precautions are necessary to protect the operated spine and help it heal properly. Normal daily activities should be started slowly and only after the surgeon confirms it is safe.
When can normal daily activities be resumed after cervical spine surgery?
Simple daily activities can usually be started within a few weeks, depending on how the patient is recovering. Activities such as driving, going back to work, travelling, and lifting heavier items may take longer. The exact recovery time depends on wound healing, improvement in muscle strength, bone fusion process, and the surgeon’s advice during follow-up visits.
When should a patient seek urgent care after cervical spine surgery?
Urgent medical care is needed if there is fever, wound discharge, severe pain, increasing weakness, new numbness, difficulty walking, or loss of bladder or bowel control. These signs should not be ignored after spine surgery. Early treatment can help prevent complications.
Share on
Request an appointment
Fill in the appointment form or call us instantly to book a confirmed appointment with our super specialist at 04048486868
Appointment request - health articles
Recent Articles