Pneumothorax: Symptoms, Causes & Treatment
PACE Hospitals
Written by: Editorial Team
Medically reviewed by: Dr. Pradeep Kiran Panchadi - Consultant Pulmonologist, Specialist in Bronchoscopy and EBUS
Overview | Epidemiology | Types | Symptoms | Causes | Risk Factors | Complications | Diagnosis | Treatment | Prevention | Hemothorax vs Pneumothorax | FAQs | When to consult a Doctor
Pneumothorax definition
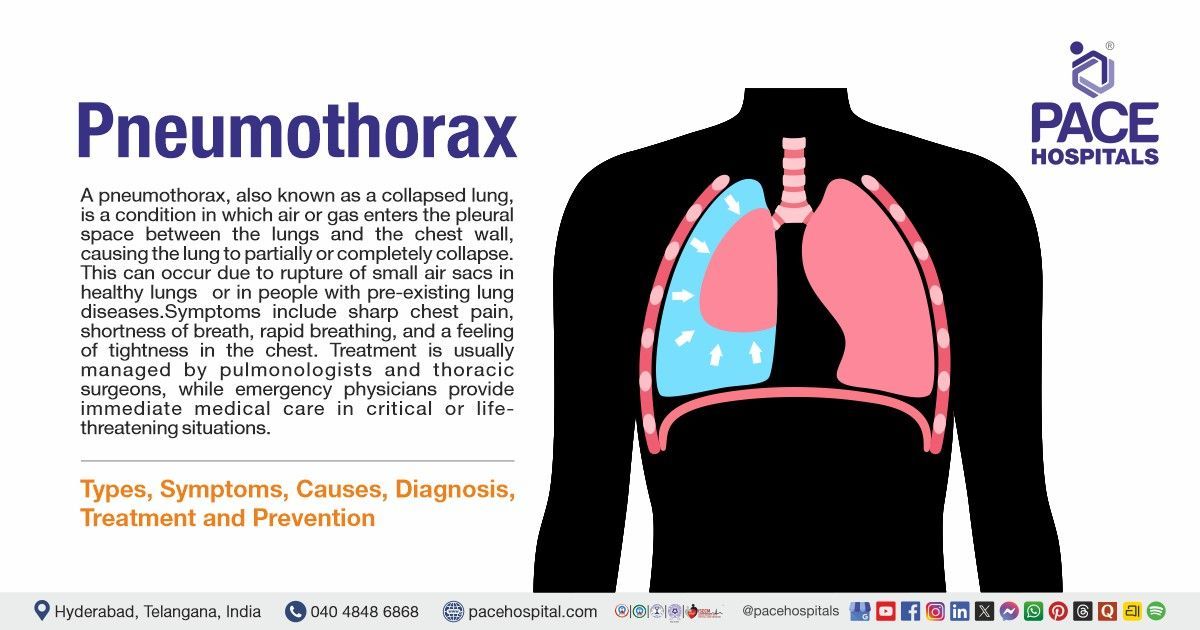
A pneumothorax, also known as a collapsed lung, is a condition in which air or gas enters the pleural space between the lungs and the chest wall, causing the lung to partially or completely collapse. This can occur due to rupture of small air sacs in healthy lungs (primary spontaneous pneumothorax) or in people with pre-existing lung diseases such as chronic obstructive pulmonary disease (COPD) or cystic fibrosis (secondary spontaneous pneumothorax). It may also develop due to chest injuries, trauma, or certain surgical procedures and medical treatments involving the lungs or chest.
Symptoms include sharp chest pain, shortness of breath, rapid breathing, and a feeling of tightness in the chest. If left untreated, it can lead to serious complications like tension pneumothorax, empyema, cardiac arrest, chronic air leaks, re-expansion pulmonary edema, infection, and high rates of recurrence.
Treatment is usually managed by pulmonologists and thoracic surgeons, while emergency physicians provide immediate medical care in critical or life-threatening situations.
Pneumothorax meaning
The term pneumothorax is derived from Greek medical terminology.
- “Pneumo-”: meaning relating to the lungs or air, derived from pneumōn (Greek for "air" or "lung").
- “-thorax”: meaning chest, from the Greek word for "chest."
“Pneumothorax” refers to the presence of air in the pleural cavity, the space between the lungs and the chest wall, leading to a collapsed lung.
Epidemiology of Pneumothorax
Pneumothorax epidemiology Worldwide
Primary spontaneous pneumothorax (PSP) has an annual incidence of approximately 7.4–18 cases per 100,000 men and 1.2–6 cases per 100,000 women, with some recent studies reporting rates of about 12.3 per 100,000 men and 2.2 per 100,000 women. A secondary spontaneous pneumothorax (SSP) occurs in about 66.3 per 100,000 men and 2 per 100,000 women. It is more common in older people who already have lung diseases like chronic obstructive pulmonary disease (COPD). PSP is much more likely to happen if you smoke, while SSP is more likely to happen if you already have a lung problem.
Pneumothorax epidemiology in India
The number of pneumothorax cases in India tends to follow world trends. Secondary spontaneous pneumothorax (SSP) mostly happens to older people who already have lung problems, while primary spontaneous pneumothorax (PSP) mostly happens to young male smokers. Unlike Western countries, where chronic obstructive pulmonary disease (COPD) is the leading cause of SSP, tuberculosis (TB) is also a major cause in India. Reliable nationwide population-based incidence data are limited. Most available information comes from hospital-based studies. These studies suggest prevalence rates like 409 cases per 100,000 hospital admissions, which is about 2–3% of all chest disease admissions. However, these rates may not be representative of the whole population.

Types of Pneumothorax
Pneumothorax can occur due to different causes and conditions and is therefore classified into several types based on its origin and characteristics. The following are the different types of pneumothorax:
- Spontaneous Pneumothorax (occurs without trauma)
- Primary Spontaneous Pneumothorax (PSP)
- Secondary Spontaneous Pneumothorax (SSP)
- Catamenial Pneumothorax
- Traumatic Pneumothorax (due to injury)
- Open Pneumothorax
- Closed Pneumothorax
- Iatrogenic Pneumothorax
- Tension Pneumothorax
Spontaneous Pneumothorax
It is a type of pneumothorax that occurs without any trauma or external injury. It happens when air collects in the pleural space spontaneously, causing partial or complete lung collapse.
- Primary Spontaneous Pneumothorax (PSP): It occurs in people with no underlying lung disease, and often affects tall, thin young adults. It is caused by rupture of small air blisters (blebs) on the lung surface.
- Secondary Spontaneous Pneumothorax (SSP): It happens in patients with pre-existing lung conditions such as COPD, cystic fibrosis, or tuberculosis. It is usually more severe and can cause significant respiratory compromise.
- Catamenial Pneumothorax: It is a rare form that occurs in women, usually within 72 hours of menstruation. It is thought to be related to endometrial tissue or hormonal changes affecting the diaphragm or pleura.
Traumatic Pneumothorax
It is a type of pneumothorax caused by chest trauma. Air enters the pleural space due to external trauma or blunt force, leading to lung collapse.
- Open pneumothorax: It is caused by a penetrating chest trauma that allows air to easily enter and exit the pleural space. It is usually referred to as a "sucking” chest wound and can cause difficulty breathing.
- Closed Pneumothorax: It is caused by blunt trauma that tears lung tissue but leaves no visible wounds. It permits air to enter the pleural space but does not communicate with the outside, resulting in lung collapse.
Iatrogenic Pneumothorax
It occurs as a complication of medical procedures such as central line insertion, lung biopsy, or mechanical ventilation. It is usually small but may need intervention depending on size and symptoms.
Tension Pneumothorax
It is a life-threatening emergency in which air gets into the pleural space but cannot exit, raising chest pressure. It puts pressure on the heart and the opposite lung, resulting in severe hypotension and respiratory failure that necessitates rapid decompression.

Pneumothorax Symptoms
A pneumothorax is the collection of air in the pleural space, causing the lung to collapse. Symptoms result from impaired lung expansion, reduced oxygen exchange, and pressure on surrounding structures. They may differ depending on the size, type, and underlying lung health. Common pneumothorax signs and symptoms include:
- Chest pain
- Dyspnea (shortness of breath)
- Tachypnea (fast breathing)
- Tachycardia (fast heartbeat)
- Dry cough
- Fatigue
- Anxiety
- Use of accessory muscles (extra effort to breathe)
- Decreased or absent breath sounds
- Hyperresonance (hollow sound when tapping the chest)
- Subcutaneous emphysema
- Hypotension
- Jugular venous distension
- Tracheal deviation
- Cyanosis (bluish skin or lips)
Chest pain: One of the most common signs of pneumothorax is sudden, sharp chest pain. It usually happens on the affected side and worsens with deep breathing or coughing. This is because the pleural lining gets irritated.
Dyspnea (shortness of breath): Shortness of breath (SOB) occurs because the collapsed lung cannot fully expand, reducing oxygen exchange. Severity depends on the size of the pneumothorax and the patient's underlying lung condition.
Tachypnea (fast breathing): As a result of the collapsed lung, the body tries to compensate for lower oxygen levels and worse circulation by breathing rapidly.
Tachycardia (fast heartbeat): The heart rate increases as the body tries to maintain adequate oxygen delivery to tissues. Tachycardia may also occur due to stress, pain, or decreased oxygenation.
Dry cough: A persistent, non-productive cough may occur because of irritation of the pleura and reduced lung expansion.
Fatigue: Reduced oxygen delivery to tissues can result in generalized weakness and tiredness. Patients may feel exhausted even with minimal physical activity.
Anxiety: Difficulty breathing and chest discomfort can cause anxiety or a feeling of distress. Low oxygen levels and activation of the sympathetic nervous system may also contribute to restlessness.
Use of accessory muscles (extra effort to breathe): Patients may use neck and chest muscles to assist breathing because the lungs cannot expand effectively. This sign indicates increased respiratory effort.
Decreased or absent breath sounds: During physical examination, breath sounds may be reduced or absent on the affected side because air in the pleural space prevents normal lung expansion.
Hyperresonance (hollow sound when tapping the chest): Percussion of the chest produces a hyperresonant or hollow sound due to excess air in the pleural space compared with normal lung tissue.
Subcutaneous emphysema: Air can escape from the pleural space into the tissues under the skin, causing swelling and a crackling sensation when touched.
Hypotension: Low blood pressure can occur in extreme situations, especially in tension pneumothorax, in which increased intrathoracic pressure compresses the heart and main blood vessels.
Jugular venous distension: Elevated pressure in the chest can impair venous return to the heart, causing the neck veins to become visibly distended.
Tracheal deviation: In tension pneumothorax, pressure from trapped air can push the trachea away from the affected side. This is a late and serious clinical sign.
Cyanosis (bluish skin or lips): Cyanosis occurs when oxygen levels in the blood become significantly reduced, leading to bluish discoloration of the lips, skin, or nail beds.

Pneumothorax Causes
Pneumothorax can occur due to several conditions that allow air to enter the pleural space between the lung and chest wall. The etiology of pneumothorax generally includes:
- Rupture of subpleural blebs or bullae
- Chronic obstructive pulmonary disease (COPD)
- Cystic fibrosis
- Pulmonary infections
- Interstitial lung diseases
- Lung malignancy (lung cancer)
- Chest trauma
- Barotrauma
- Medical procedures
Rupture of subpleural blebs or bullae: Subpleural blebs or bullae are small air-filled sacs that form on the surface of the lungs. When these sacs rupture, air leaks into the pleural space, causing the lung to partially or fully collapse. This mechanism is the most common cause of primary spontaneous pneumothorax in people without underlying lung illness.
Chronic obstructive pulmonary disease (COPD): In COPD, especially emphysema, the lung tissue becomes damaged and fragile. The destruction of alveolar walls can form bullae that may rupture, allowing air to escape into the pleural cavity and causing a pneumothorax.
Cystic fibrosis: Cystic fibrosis leads to thick mucus accumulation and chronic lung infections. These changes damage lung tissue and create areas of weakness, increasing the risk of air leakage and pneumothorax.
Pulmonary infections: Severe lung infections such as tuberculosis or pneumocystis pneumonia can damage lung tissue and form cavities. When these weakened areas rupture, air can enter the pleural space and result in pneumothorax.
Interstitial lung diseases: Diseases that cause scarring and fibrosis of lung tissue make the lungs stiff and fragile. Structural changes in the lungs can predispose them to rupture, allowing air to escape into the pleural cavity.
Lung malignancy (lung cancer): Tumors in the lungs may invade or destroy lung tissue and airways. This damage can create abnormal connections between the airways and pleural space, resulting in pneumothorax.
Chest trauma: Blunt or penetrating injuries to the chest, such as rib fractures, stab wounds, or gunshot injuries, can puncture the lung. This allows air from the lungs to escape into the pleural space.
Barotrauma: It occurs when excessive pressure damages the lung tissue. It may occur during mechanical ventilation, scuba diving, or rapid pressure changes, leading to alveolar rupture and pneumothorax.
Medical procedures: Certain medical procedures affecting the chest or lungs may unintentionally introduce air into the pleural space. Thoracentesis, lung biopsy, central venous catheter insertion, and bronchoscopy are some examples of procedures.

Pneumothorax Risk Factors
Several factors increase the likelihood of developing a pneumothorax by weakening lung tissue or increasing the risk of air leakage into the pleural space. The following are the risk factors of pneumothorax:
- Cigarette smoking
- Male sex
- Tall and thin body habitus
- Underlying lung diseases
- Previous history of pneumothorax
- Family history of pneumothorax
- Genetic connective tissue disorders
- Mechanical ventilation
- Sudden pressure changes (such as scuba diving or high-altitude exposure)
Cigarette smoking: Smoking significantly increases the risk of pneumothorax because it damages lung tissue and promotes the formation of subpleural blebs. The risk increases with the number of cigarettes smoked and is several times higher in smokers compared with non-smokers.
Male sex: Primary spontaneous pneumothorax occurs more frequently in males than in females. Hormonal and anatomical differences, along with a higher prevalence of smoking in males, may contribute to this increased risk.
Tall and thin body habitus: Individuals who are tall and thin have a higher risk of spontaneous pneumothorax. This may be due to greater pressure differences in the upper parts of the lungs, which can promote the formation and rupture of apical blebs.
Underlying lung diseases: Conditions such as chronic obstructive pulmonary disease (COPD), cystic fibrosis, tuberculosis, and interstitial lung disease can weaken lung tissue. These diseases increase the likelihood of air leakage into the pleural space.
Previous history of pneumothorax: People who have had pneumothorax in the past are at increased risk of recurrence. Structural abnormalities in the lungs or persistent blebs may predispose them to repeated episodes.
Family history of pneumothorax: A family history may increase the risk due to inherited structural abnormalities of the lungs or genetic predisposition to bleb formation.
Genetic connective tissue disorders: Marfan syndrome and Ehlers-Danlos syndrome are two conditions that impact connective tissue strength. These disorders can damage lung tissues and raise the risk of pneumothorax.
Mechanical ventilation: Positive pressure ventilation can increase pressure within the lungs. Excessive airway pressure may cause alveolar rupture, allowing air to leak into the pleural space.
Sudden pressure changes: Activities such as scuba diving, flying, or exposure to high altitude involve rapid changes in pressure. These changes can lead to lung expansion and rupture of weak areas in the lung.

Pneumothorax Complications
Complications may develop if the condition is severe, left untreated, or associated with trauma or underlying lung disease. These complications mainly affect the respiratory and cardiovascular systems and may worsen the patient’s clinical condition if not managed promptly. The complications of pneumothorax include:
- Respiratory failure or respiratory arrest
- Cardiac arrest
- Pyopneumothorax
- Empyema
- Re-expansion pulmonary edema
- Pneumopericardium
- Pneumoperitoneum
- Pneumohemothorax
- Bronchopleural fistula
- Injury to the neurovascular bundle during tube thoracostomy
- Pain and local skin infection at the tube thoracostomy site
Respiratory failure or respiratory arrest: Severe pneumothorax can cause major lung collapse, leading to impaired oxygen exchange. If not treated, the lack of oxygen may lead to respiratory failure or complete respiratory arrest.
Cardiac arrest: In life-threatening cases such as tension pneumothorax, increased intrathoracic pressure compresses the heart and major vessels. This can severely reduce cardiac output and may ultimately lead to cardiac arrest.
Pyopneumothorax: It occurs when both air and pus accumulate in the pleural cavity. It usually results from infection within the pleural space and may require drainage and antibiotic therapy.
Empyema: It refers to the collection of pus in the pleural space due to infection. It can develop after prolonged pneumothorax, chest tube placement, or secondary bacterial infection.
Re-expansion pulmonary edema: This complication can occur after rapid re-expansion of a collapsed lung following drainage. It results in fluid accumulation in the lung tissue and can cause severe breathing difficulty.
Pneumopericardium: It is the presence of air within the pericardial sac surrounding the heart. It may occur due to trauma or air leakage from the lungs and can impair normal cardiac function.
Pneumoperitoneum: It refers to the presence of air in the abdominal cavity. In rare cases of pneumothorax, air may track through tissue planes into the peritoneal cavity.
Pneumohemothorax: It is the buildup of both air and blood in the pleural cavity. It frequently arises after chest trauma and can cause severe respiratory impairment.
Bronchopleural fistula: This condition involves an abnormal connection between the bronchial tree and the pleural space. It can lead to persistent air leaks and difficulty in lung re-expansion.
Injury to the neurovascular bundle during tube thoracostomy: During chest tube insertion, nearby nerves and blood vessels may be accidentally damaged. This can result in bleeding, nerve injury, or long-term pain.
Pain and local skin infection at the tube thoracostomy site: Chest tube placement can cause discomfort and irritation at the insertion site. Poor wound care or prolonged tube placement may result in local skin infection.
Pneumothorax Diagnosis
Pneumothorax is diagnosed using clinical symptoms, a physical examination, and imaging tests. Early identification is critical for avoiding respiratory problems. Bedside evaluation, along with radiological confirmation, helps determine the presence, size, and type of pneumothorax, guiding appropriate treatment.
The diagnostic process typically includes the following steps:
- Medical history
- Physical examination
- Initial imaging – Chest X-ray
- Thoracic ultrasound
- Pulse oximetry
- Laboratory investigations
- Arterial Blood Gas (ABG) analysis
- Complete blood count (CBC)
- Computed tomography (CT) scan
- Bronchoscopy (if indicated for etiology)
- Electrocardiogram (ECG)
- Ultrasonography E-FAST (extended focused abdominal sonography for trauma) exam
- Assessment of pneumothorax size
Pneumothorax Treatment
The treatment of pneumothorax is tailored to the type, size, and severity of the pneumothorax, as well as the patient’s clinical condition. The main goal of treatment is to allow the lung to re-expand and to prevent complications such as respiratory failure or recurrence. The following are the treatment options for pneumothorax:
- Initial care and stabilization
- Administer oxygen (high-flow if stable to help air resorption)
- Check patient stability and monitor vital signs
- Small pneumothorax (conservative treatment)
- Observation and monitoring of the patient’s condition.
- Supplemental oxygen is given to promote air resorption.
- Repeat imaging (e.g., chest X-ray) to track progress.
- Moderate pneumothorax (needle or pigtail drainage)
- Perform needle aspiration or small pigtail catheter if needed
- Follow-up imaging to ensure improvement
- Large or recurrent pneumothorax (chest tube)
- Insert chest tube if symptomatic, >2–3 cm, or traumatic
- Prefer a small-bore tube initially.
- Monitor drainage and consider antibiotics if needed.
- Repeat imaging to check progress
- Persistent or recurrent pneumothorax (surgery)
- Surgery if leaks persist >5 days or pneumothorax recurs
- Options: Video-assisted thoracic surgery (VATS) with or without pleurodesis, thoracotomy required rarely.
- Monitor patient after surgery
- Tension pneumothorax (emergency)
- Immediate needle decompression at 2nd intercostal space, midclavicular line
- Insert chest tube after decompression
- Pain control and support
- Use NSAIDs, opioids, local anaesthetics, or intercostal blocks
- Encourage chest physiotherapy
Why Choose PACE Hospitals?
Expert Super Specialist Doctors
Advanced Diagnostics & Treatment
Affordable & Transparent Care
24x7 Emergency & ICU Support

Pneumothorax Prevention
Pneumothorax prevention is important, especially for people at risk, such as those with lung disease or a history of lung collapse. Early precautions and timely care can reduce the risk and complications. The following are the preventive measures for pneumothorax:
- Smoking cessation
- Lifestyle and activity modifications
- Patient education on early symptoms
- Avoidance of high risk procedures without imaging guidance
- Surgical measures to prevent recurrence
- Pleurodesis
- Follow up and long term monitoring
Smoking cessation: Quitting smoking significantly reduces the risk of recurrent spontaneous pneumothorax and improves overall lung health. Smoking is a well recognized risk factor for the initial occurrence and recurrence of pneumothorax.
Lifestyle and activity modifications: Patients need to avoid activities that involve sudden or extreme changes in pressure, such as scuba diving, high altitude travel, and flying shortly after a pneumothorax until full resolution and medical clearance.
Patient education on early symptoms: Educating patients to recognize early signs, like sudden chest pain or shortness of breath, encourages prompt medical attention, which can prevent worsening or complications.
Avoidance of high risk procedures without imaging guidance: For procedures like central venous cannulation, using ultrasound guidance reduces the risk of causing an iatrogenic pneumothorax.
Surgical measures to prevent recurrence: After recurrent pneumothorax or in high risk individuals, surgical intervention such as pleurectomy, pleurodesis, or bleb removal (often via VATS) is effective in preventing further episodes. Surgical prevention significantly lowers recurrence rates compared to conservative management alone.
Pleurodesis: Chemical or mechanical pleurodesis creates pleural adhesions that obliterate the pleural space, reducing the likelihood of air re accumulation and recurrence.
Follow up and long term monitoring: Regular follow up with a pulmonologist, especially after an initial pneumothorax or surgery, helps monitor lung health and detect early signs of recurrence.
Difference between Hemothorax and Pneumothorax
Hemothorax vs Pneumothorax
Hemothorax and pneumothorax are pleural cavity abnormalities that are commonly related with chest trauma or underlying lung illnesses. Although they may have similar respiratory symptoms, they differ in terms of the substance collected in the pleural space and the clinical implications. Understanding the differences between them is essential for accurate diagnosis and appropriate management.
The following table highlights the key differences between hemothorax and pneumothorax:
| Feature | Hemothorax | Pneumothorax |
|---|---|---|
| Meaning | Presence or collection of blood in the pleural cavity between the lung and chest wall. | Presence or collection of air in the pleural cavity between the lung and chest wall. |
| Common Causes | Chest trauma, rib fracture, lung injury, thoracic surgery, rupture of blood vessels. | Chest injury, rupture of lung blebs, lung diseases, and mechanical ventilation. |
| Contents in the Pleural Space | The pleural space is filled with blood due to damage to blood vessels, lungs, or the chest wall. The collected blood compresses the lung and reduces its ability to expand normally during breathing. | The pleural space is filled with air that enters from the lung or through a chest wall injury. The trapped air increases pressure in the pleural cavity and causes partial or complete collapse of the lung. |
| Breath Sounds | Breath sounds are decreased or absent on the affected side due to compression by blood. | Breath sounds are absent or markedly reduced because air prevents lung expansion. |
| Percussion Note | Dull percussion note due to the presence of fluid (blood). | Hyper-resonant percussion note due to the presence of air. |
| Treatment | Chest tube drainage, blood replacement, and sometimes surgery. | Needle decompression or chest tube insertion to remove air and re-expand the lung. |
Comparison of Pneumothorax X-ray vs Normal
A chest X-ray is used to examine the lungs and pleural space for abnormalities. It helps identify conditions like pneumothorax by showing a collapsed lung and trapped air compared to a normal X-ray.
Pneumothorax X-ray:
- There is a visible line of the collapsed lung (visceral pleura), but no lung marks beyond it.
- The affected side appears more radiolucent (darker) due to trapped air.
- In tension pneumothorax, the mediastinum may migrate to the other side
- The damaged side of the diaphragm may appear flat.
Normal Chest X-ray:
- Lung fields show uniform lung markings throughout.
- Both lungs are fully expanded with no collapsed areas or abnormal air collections.
- The mediastinum and diaphragm are in normal positions.
Frequently asked questions (FAQs) ON Pneumothorax
What is pneumothorax?
Pneumothorax, commonly called a collapsed lung, is a condition in which air accumulates in the pleural space between the lung and chest wall, causing the lung to partially or completely collapse. It may occur spontaneously, due to lung diseases such as COPD or asthma, or as a result of chest injury or ruptured air blisters (blebs). Common symptoms include sudden, sharp chest pain, shortness of breath, and difficulty breathing. Treatment depends on severity and may involve observation, needle aspiration, or chest tube insertion.
Can pneumothorax cause death?
Yes, pneumothorax can be life-threatening, especially in cases of tension pneumothorax. In this form, air gets trapped in the pleural space, creating increased pressure that can compress the lung and major blood vessels, severely impairing respiratory function and blood circulation. Tension pneumothorax is a medical emergency and requires immediate intervention, like needle decompression and chest tube insertion, to prevent fatal outcomes. Other forms of pneumothorax, if left untreated, might result in problems such as recurrence, respiratory failure, or death.
How does COPD cause pneumothorax?
COPD increases the likelihood of pneumothorax due to the destruction of lung tissue and the formation of bullae (air-filled sacs). These bullae can rupture, enabling air to escape into the pleural space and cause a pneumothorax. This is known as secondary spontaneous pneumothorax (SSP), and it is more likely in people with severe emphysema or a long smoking history.
The damaged lung tissue in COPD patients makes it harder for the lung to re-expand after air is drained. This increases the risk of recurrent pneumothorax, requiring more aggressive management like chest tube placement or even surgery.
Who is most at risk for pneumothorax?
People at higher risk for pneumothorax include young, tall, thin males, especially for primary spontaneous pneumothorax (PSP). People who smoke are more likely to get this disease because smoking damages lung tissue, which can cause blebs that can burst. Patients with underlying lung diseases, such as COPD, asthma, interstitial lung disease, or cystic fibrosis, are also at increased risk for secondary pneumothorax.
People undergoing invasive medical procedures, such as lung biopsy or central venous catheter placement, are also at risk for iatrogenic pneumothorax.
How can pneumothorax be prevented?
Prevention of a pneumothorax (collapsed lung) includes quitting smoking or vaping, avoiding sudden changes in air pressure (such as scuba diving or high-altitude flying) if you are at risk, managing existing lung conditions like COPD or asthma, and protecting the chest from injury. For individuals who have experienced a prior collapse, medical interventions such as pleurodesis can help prevent it from happening again.
Which type of pneumothorax is the most serious?
Tension pneumothorax is the most serious type of pneumothorax. In this case, air builds up in the pleural space under pressure and cannot escape. This puts strain on the heart and lungs, which makes it hard to breathe and circulate blood. This is a medical emergency that needs rapid needle decompression and then chest tube placement to relieve pressure.
If not treated, tension pneumothorax can cause the heart to stop beating, respiratory failure, and death.
Can pneumothorax cause pleural effusion?
While pneumothorax involves air in the pleural space, pleural effusion is the accumulation of fluid in the same space. These two conditions can coexist, especially in the case of traumatic pneumothoraxes. After a trauma-related pneumothorax, blood may accumulate alongside air, resulting in hemopneumothorax, a condition that can also lead to pleural effusion.
Infection, inflammation, or surgical interventions after a pneumothorax can also cause pleural fluid accumulation, which complicates treatment. Both conditions may require drainage to remove fluid and air from the pleural space and ensure proper lung re-expansion.
How does tracheostomy cause pneumothorax?
A tracheostomy can lead to pneumothorax if the tracheostomy tube is inserted incorrectly or if there is trauma to the airway or pleura during the procedure. The air from the airway can escape into the pleural space, causing the lung to collapse. This is a known iatrogenic cause of pneumothorax.
The risk is higher in patients with pre-existing lung conditions or those who are critically ill. If pneumothorax occurs, it typically requires needle decompression or chest tube insertion to relieve the trapped air and prevent further complications.
What is the main cause of pneumothorax?
The primary cause of pneumothorax is spontaneous rupture of blebs or bullae (air-filled sacs) in the lungs, especially in patients with lung disease such as COPD. It can also occur spontaneously in healthy individuals, particularly young, tall, thin males (Primary Spontaneous Pneumothorax or PSP). Trauma (e.g., rib fractures) and medical procedures like central line insertion or lung biopsy are also significant causes.
Smoking is a major risk factor for pneumothorax, especially in patients with underlying lung disease. It accelerates lung tissue damage, leading to the formation of blebs and increasing the risk of pneumothorax.
What happens if a pneumothorax goes untreated?
If left untreated, pneumothorax can lead to progressive lung collapse and, in the event of tension pneumothorax, circulatory failure and death. Air trapped in the pleural space can cause the lungs to remain deflated, leading to respiratory failure. Furthermore, an untreated pneumothorax can result in recurring occurrences in people who already have lung problems.
Pleural effusion or infection are examples of complications that might make the condition more difficult to control. Immediate treatment is required to prevent long-term lung damage and improve outcomes.
Can a pneumothorax cause brain damage?
While pneumothorax itself doesn’t cause brain damage, severe hypoxia (low oxygen levels) caused by untreated or severe pneumothorax can lead to anoxic brain injury. Prolonged low oxygen levels can deprive the brain of required oxygen, resulting in brain damage and neurological dysfunction. Prompt treatment to restore oxygenation can prevent this.
However, mild pneumothorax typically does not result in brain injury unless there is a significant delay in treatment, leading to prolonged hypoxia.
Can a pneumothorax cause permanent damage?
When treated promptly, most pneumothorax instances recover without causing long-term damage. Recurrent pneumothorax or a large untreated pneumothorax can result in lung scarring, pleural adhesions, and decreased lung function over time. Such long-term lung damage may cause ongoing breathing difficulties and raise the risk of future pneumothorax episodes.
In the worst cases, lung tissue can be destroyed, which can cause long-term breathing problems or the complete loss of lung function.
Is pneumothorax a rare disease?
Pneumothorax is not considered a rare disease, but it is relatively uncommon in the general population. The incidence is about 7–24 cases per 100,000 people per year in men and 1–9 cases per 100,000 people per year in women, depending on the population studied. However, the risk is significantly higher in certain groups, like smokers and patients with chronic lung diseases such as chronic obstructive pulmonary disease (COPD).
Can anxiety cause pneumothorax?
Anxiety does not directly cause pneumothorax. However, it can result in hyperventilation, which may worsen breathing difficulties in people with existing lung conditions. While this can increase the risk of complications, anxiety itself does not trigger a pneumothorax.
When to consult a doctor for pneumothorax?
Consult a doctor for pneumothorax if you experience sudden chest pain, shortness of breath, or difficulty breathing. Signs that need attention include:
- Sharp chest pain
- Rapid breathing
- Bluish lips or fingertips
- Dizziness, fainting, or rapid heartbeat
- Worsening shortness of breath (SOB) over time
If these symptoms occur, it is important to seek emergency medical care immediately. A general care physician, pulmonologist, or pneumothorax specialist can provide the best evaluation, perform imaging tests, and recommend appropriate pneumothorax treatment such as observation, needle aspiration, chest tube placement, or surgery to prevent complications.
Share on
Request an appointment
Fill in the appointment form or call us instantly to book a confirmed appointment with our super specialist at 04048486868
Appointment request - health articles
Recent Articles