
Successful Splenectomy with Proximal Splenorenal Shunt for Extrahepatic Portal Venous Obstruction
PACE Hospitals
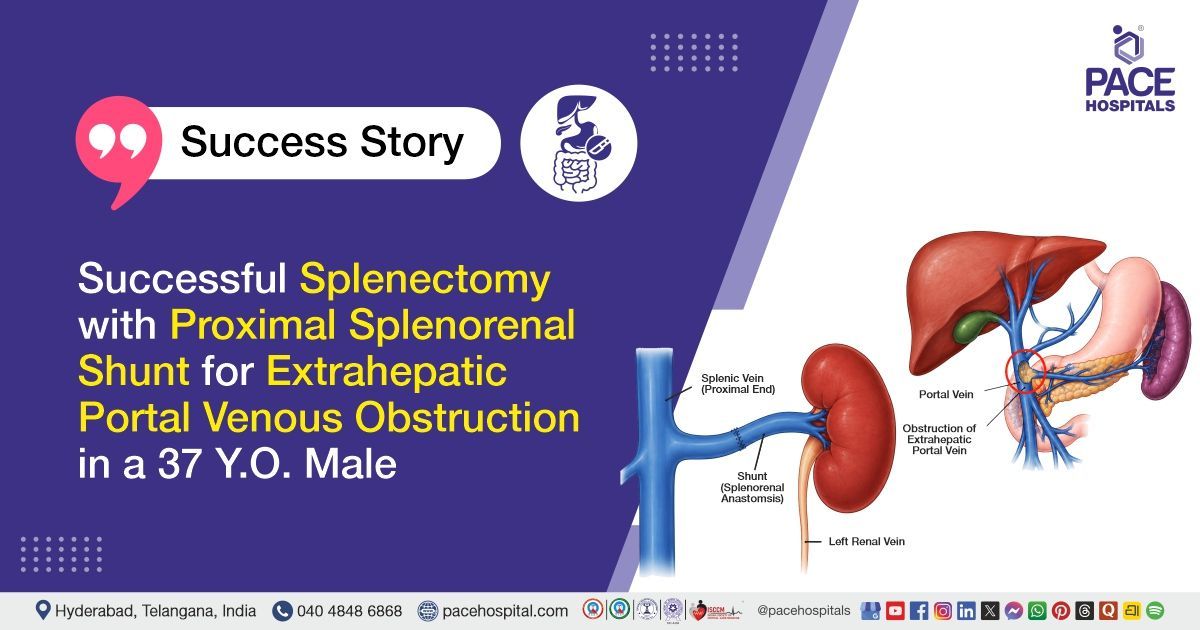
PACE Hospitals’ expert Surgical Gastroenterology team successfully performed Splenectomy with Proximal Splenorenal Shunt and Liver Biopsy on a 37-year-old male patient diagnosed with Extra Hepatic Portal Venous Obstruction (EHPVO), porto-pulmonary hypertension, hepatopulmonary syndrome, and hypersplenism. The aim of the procedure was to reduce portal hypertension, improve blood flow through the portal venous system, relieve hypersplenism-related complications, and prevent further complications such as variceal bleeding and worsening portal hypertension.
Chief Complaints
A 37-year-old male patient with a body mass index (BMI) of 20 presented to the Surgical Gastroenterology Department at PACE Hospitals, Hitech City, Hyderabad, with complaints of shortness of breath and recurrent syncopal attacks for the past 6 months. There was no similar history in the past. Further evaluation revealed features suggestive of porto-pulmonary hypertension associated with portal hypertension.
Past Medical History
The patient had no significant prior surgical history. Evaluation before admission revealed chronic portal vein thrombosis with collaterals, early esophageal and fundal varices, and features suggestive of chronic liver disease with caudate lobe hypertrophy. Transjugular liver biopsy performed earlier showed mild central venous dilation.
On Examination
On examination, the patient was conscious, coherent, oriented and hemodynamically stable. Clinical evaluation and imaging findings were suggestive of portal hypertension with massive splenomegaly. Intraoperative findings later revealed an enlarged spleen measuring approximately 20 cm extending into the epigastric and left lumbar regions, along with large perigastric, periportal, and peripancreatic collaterals. No ascites was noted intraoperatively, and the liver appeared grossly normal with mild left lobe atrophy.
Diagnosis
Upon admission to PACE Hospitals, the Surgical Gastroenterology team conducted a detailed clinical evaluation of the patient’s complaints of shortness of breath and recurrent syncopal attacks. A comprehensive review of the patient’s medical history, systemic examination, and diagnostic workup was performed to identify the underlying cause of portal hypertension and associated cardiopulmonary complications.
Upper gastrointestinal endoscopy revealed early esophageal and fundal varices suggestive of portal hypertension. Contrast-enhanced computed tomography (CECT) demonstrated chronic portal vein thrombosis with extensive periportal collaterals, chronic liver disease changes with caudate lobe hypertrophy, and massive splenomegaly. Liver Doppler evaluation confirmed chronic thrombosis of the portal vein and its branches with collateral formation, while the splenorenal shunt and superior mesenteric vein were patent.
Cardiac evaluation with 2D echocardiography showed mild pulmonary arterial hypertension with mildly dilated right atrium and left atrium, suggestive of porto-pulmonary hypertension. Arterial blood gas analysis demonstrated reduced oxygenation consistent with hepatopulmonary syndrome. Laboratory investigations revealed thrombocytopenia, anemia, neutrophilic leukocytosis, and mild liver function abnormalities associated with hypersplenism and portal hypertension.
Based on the confirmed diagnosis, the patient was advised to undergo Extra Hepatic Portal Venous Obstruction (EHPVO) with Hypersplenism and Portal Hypertension Treatment in Hyderabad, India, under the expert care of the Surgical Gastroenterology Department.
Medical Decision Making (MDM)
After a detailed consultation with Dr. CH Madhusudan, Senior Consultant Surgical Gastroenterologist and Liver Transplant Surgeon, along with the team, including Dr. Suresh Kumar S, Consultant Surgical Gastroenterologist, a comprehensive clinical, radiological, and hepatological evaluation was carried out to determine the most appropriate management plan for the patient presenting with shortness of breath and recurrent syncopal attacks associated with portal hypertension.
A detailed review of investigations, including upper gastrointestinal endoscopy, contrast-enhanced CT abdomen, liver Doppler, 2D echocardiography, arterial blood gas analysis, liver function tests, coagulation profile, complete blood picture, renal function tests, and liver biopsy findings, was performed. The evaluation confirmed Extra Hepatic Portal Venous Obstruction (EHPVO) with chronic portal vein thrombosis, extensive periportal collaterals, hypersplenism, porto-pulmonary hypertension, hepatopulmonary syndrome, esophageal and fundal varices, and massive splenomegaly.
Based on the multidisciplinary assessment and considering the risks of progressive portal hypertension, variceal bleeding, worsening hypersplenism, and cardiopulmonary complications, surgical intervention was planned. It was determined that splenectomy with proximal splenorenal shunt and liver biopsy was the most appropriate treatment to provide effective portal decompression, reduce splenic sequestration-related complications, improve portal venous blood flow, and help prevent further disease progression.
The patient and family members were counselled in detail regarding the diagnosis, surgical procedure, expected benefits, possible postoperative complications, including bleeding, infection, thrombosis, shunt-related complications, and the need for long-term follow-up and continued multidisciplinary care.
Surgical Procedure
Following the decision, the patient was scheduled to undergo Splenectomy with Proximal Splenorenal Shunt and Liver Biopsy in Hyderabad at PACE Hospitals under the expert care of the Surgical Gastroenterology Department.
The procedure involved the following steps:
- Surgical Access and Exposure: After induction of anaesthesia and standard aseptic preparation, the abdomen was opened and adequate exposure of the upper abdominal region was achieved. Intraoperative assessment revealed a massively enlarged spleen measuring approximately 20 cm extending into the epigastric and left lumbar regions, along with extensive perigastric, periportal, and peripancreatic collateral vessels. The liver appeared grossly normal, with mild atrophy of the left lobe and no evidence of ascites.
- Splenectomy: All splenic attachments were carefully dissected and divided. The enlarged spleen, along with associated hilar structures, was mobilized and splenectomy was performed with meticulous control of vascular collaterals and hemostasis. Multiple enlarged collaterals and lymph nodes around the splenic hilum were identified during the procedure.
- Proximal Splenorenal Shunt Formation: The splenic vein, which was noted to be dilated, was carefully dissected and prepared for shunt creation. A proximal splenorenal shunt was then performed by creating an end-to-side anastomosis between the splenic vein and the left renal vein to decompress the portal venous system and reduce portal hypertension-related complications.
- Liver Biopsy and Hemostasis: Liver biopsy samples were obtained from both lobes of the liver for histopathological evaluation. Following completion of the shunt procedure, meticulous hemostasis was secured, and the operative field was inspected for bleeding or shunt-related complications.
- Completion and Closure: After confirming satisfactory shunt flow and hemodynamic stability, abdominal closure was performed in layers under standard surgical precautions.
Postoperative Care
During the postoperative period, the patient was closely monitored and received supportive management for hemodynamic stabilization, maintenance of fluid and electrolyte balance, infection prevention, anticoagulation support for shunt patency, pain management, and gastric protection. On postoperative day 2, the patient developed high-grade fever, following which cultures were sent, and infection prevention therapy was upgraded based on culture findings.
Further evaluation with contrast-enhanced CT abdomen demonstrated a patent splenorenal shunt with mild narrowing due to external compression by adjacent postoperative hematoma. Multiple postoperative hematomas were noted in the retropancreatic and pararenal regions, and the patient was managed conservatively with close monitoring and supportive treatment.
Histopathological examination of the liver biopsy showed changes related to abnormal blood flow in the liver, while the spleen showed enlargement with congestion and fibrosis due to long-standing portal hypertension and hypersplenism.
The patient showed gradual clinical improvement during the hospital stay and remained hemodynamically stable. Supportive care, including hydration, nutritional support, and symptomatic management, was continued throughout recovery. The patient tolerated treatment well and was discharged in stable condition with follow-up advice and postoperative precautions.
Discharge Medications
Upon discharge, the patient was prescribed medications for anticoagulation support, prevention of postoperative infection, gastric protection, liver support, nutritional supplementation, pain relief, bowel regulation, and prevention of thrombotic complications. Supportive medications were advised to promote postoperative recovery and maintain shunt patency.
Advice on Discharge
The patient was advised to avoid strenuous physical activities and follow proper postoperative wound care with regular dressing changes. He was counselled regarding adequate hydration, nutritional support, medication adherence, and the importance of regular follow-up for monitoring shunt function and overall recovery.
Emergency Care
The patient was advised to contact the emergency ward at PACE Hospitals in case of fever, abdominal pain, vomiting, chest pain, bleeding, breathing difficulty, or any worsening symptoms requiring urgent medical attention.
Review and Follow-up Notes
The patient was advised to return for a follow-up visit with the Surgical Gastroenterologist in Hyderabad at PACE Hospitals after 3 days for postoperative evaluation, wound assessment, and continued monitoring of recovery and shunt status.
Conclusion
This case highlights the successful management of Extra Hepatic Portal Venous Obstruction (EHPVO) with porto-pulmonary hypertension, hepatopulmonary syndrome, and hypersplenism in a 37-year-old male patient. The patient underwent successful splenectomy with proximal splenorenal shunt and liver biopsy under the expert care of the Surgical Gastroenterology team. Postoperative recovery was uneventful with gradual clinical improvement, and the patient was discharged in stable condition with follow-up advice for continued monitoring and long-term management.
Surgical Management of Portal Hypertension Due to Extra-Hepatic Portal Venous Obstruction (EHPVO)
Extrahepatic Portal Venous Obstruction (EHPVO) is a condition in which blockage of the portal vein leads to increased pressure in the portal venous system, resulting in complications such as splenomegaly, hypersplenism, varices, and portal hypertension-related symptoms. Detailed evaluation using imaging studies such as Doppler ultrasound, CT scan, endoscopy, liver biopsy, and cardiac assessment helps the Surgical gastroenterologist / Surgical gastroenterology doctor determine the severity of the disease and guide appropriate treatment planning.
Surgical management aims to decompress the portal venous system, reduce complications related to portal hypertension, and improve blood flow through alternate venous pathways. Procedures such as splenectomy with proximal splenorenal shunt help reduce splenic congestion, manage hypersplenism, and lower portal pressure. Postoperative care involves close monitoring for bleeding, infection, thrombosis, shunt patency, and recovery progress. Regular follow-up and long-term monitoring remain important for maintaining liver health, preventing complications, and improving overall quality of life.
Frequently Asked Questions (FAQs)
What is Extra Hepatic Portal Venous Obstruction (EHPVO)?
Extrahepatic portal venous obstruction is a condition where the portal vein, which carries blood to the liver, becomes blocked outside the liver. This blockage increases pressure in the portal venous system and leads to portal hypertension. Over time, it can cause an enlarged spleen, varices, and blood flow abnormalities.
Why is splenectomy performed in portal hypertension patients?
Splenectomy is performed when the spleen becomes excessively enlarged and starts destroying blood cells, a condition called hypersplenism. Removal of the spleen helps improve blood counts and reduce complications related to portal hypertension. It may also reduce abdominal discomfort caused by massive splenomegaly. In selected patients, it is combined with shunt surgery for better pressure control.
What precautions should be followed after splenectomy and splenorenal shunt surgery?
Patients are usually advised to avoid strenuous activities during recovery and follow proper wound care instructions. Regular follow-up visits and imaging studies are important to monitor shunt function and healing. Adequate hydration, healthy nutrition, and medication compliance are also essential. Any fever, severe abdominal pain, or breathing difficulty should be reported immediately.
What is a proximal splenorenal shunt, and how does it help?
A proximal splenorenal shunt is a surgical procedure that redirects blood flow from the splenic vein to the left renal vein. This helps reduce pressure in the portal venous system. The procedure lowers the risk of variceal bleeding and relieves complications related to portal hypertension. It also helps improve blood circulation around the liver.
Why was a liver biopsy performed in this patient?
A liver biopsy was performed to assess the liver tissue and identify any underlying liver disease or vascular abnormalities. Even when imaging appears normal, biopsy helps confirm microscopic changes within the liver. In this patient, it helped identify features of portosinusoidal vascular disease. The biopsy findings also supported long-term treatment planning.
Why did the patient develop fainting episodes and breathing difficulty?
The patient developed these symptoms due to complications associated with portal hypertension, including porto-pulmonary hypertension and hepatopulmonary syndrome. These conditions can affect blood flow and oxygen exchange in the lungs. Reduced oxygen delivery may lead to breathlessness and fainting episodes.
What lifestyle precautions should be followed after portal hypertension surgery?
Patients are generally advised to avoid heavy lifting and strenuous physical activity during recovery. Following a balanced diet, maintaining hydration, and attending regular medical follow-up visits are important. Smoking and alcohol intake should be avoided. Long-term monitoring helps detect complications early and supports better recovery outcomes.
How long does recovery take after splenectomy and shunt surgery?
Recovery time varies depending on the patient’s overall condition and postoperative healing. Most patients gradually recover over several weeks with proper rest and medical care. Regular wound care, medications, and follow-up evaluations are important during this period. Activity levels are usually increased gradually based on recovery progress.
Why does portal hypertension lead to enlarged veins in the food pipe?
When pressure in the portal venous system increases, blood tries to bypass the blockage through alternate veins. This causes enlargement of the veins in the food pipe and stomach, known as varices. These veins are fragile and may bleed if untreated.
What are the risks of delayed treatment in portal vein obstruction?
Delayed treatment can increase the risk of severe portal hypertension, internal bleeding from varices, worsening hypersplenism, and progressive cardiopulmonary complications. Long-standing portal vein obstruction may also affect overall quality of life and nutritional status. Timely treatment helps prevent life-threatening complications and improves long-term outcomes.
Share on
Request an appointment
Fill in the appointment form or call us instantly to book a confirmed appointment with our super specialist at 04048486868
Appointment request - health articles
Recent Articles










