
Insulin Resistance: A Cause of Worry for Pre-Diabetic and Diabetic Patients
PACE Hospitals
What Is Insulin Resistance?
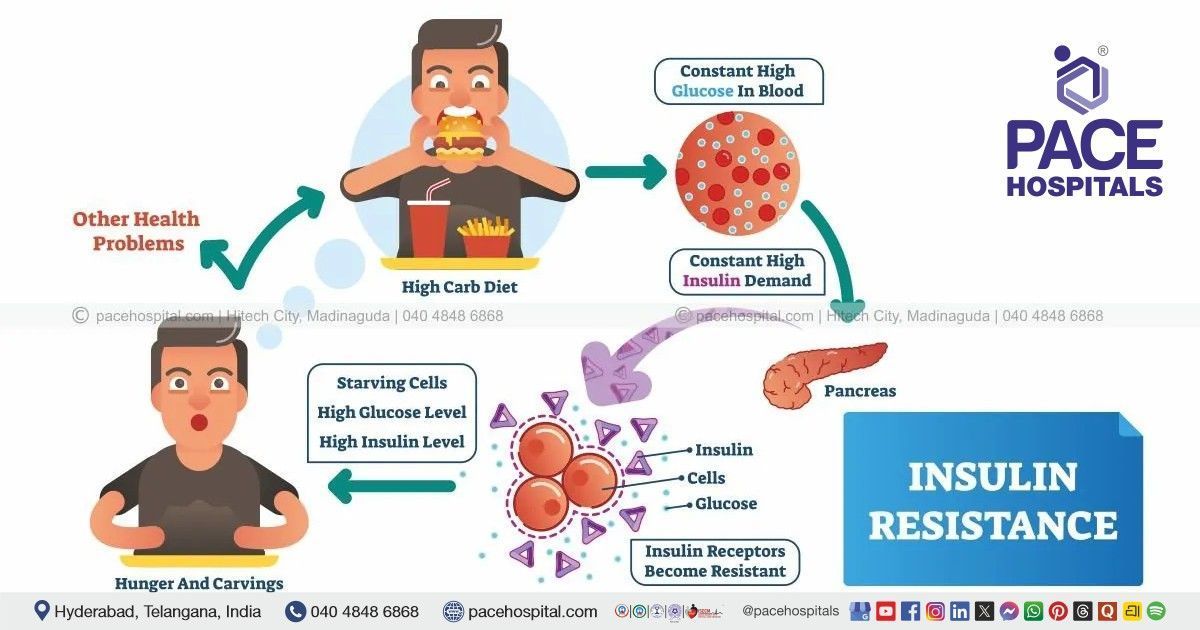
Insulin resistance occurs when body cells, particularly in muscle, liver, and fat tissue, respond inadequately to insulin. Insulin is the hormone responsible for allowing glucose to enter cells and be used for energy. When resistance develops, the pancreas compensates by producing more insulin to maintain normal blood sugar levels.
Over time, this compensatory mechanism becomes insufficient. Blood glucose levels begin to rise, leading to prediabetes and eventually type 2 diabetes if the underlying resistance is not addressed. Insulin resistance also affects fat metabolism, inflammation, and vascular health, making it a systemic metabolic disorder rather than a glucose-only issue.
In the present era of having diet fads and eating excessive junk foods, lack of physical activity, stressful life, we have been observing an increased incidence of various lifestyle disorders like obesity, metabolic syndrome, PCOS in all age groups. One such condition of major concern to not only physicians but dermatologists as well is insulin resistance which is a predictor for pre-diabetic / diabetic state.
Now Let's Talk about Why Insulin Resistance is a Cause of Worry to a Dermatologist!
When a patient walks in for a consultation with signs such as dark coarse thick skin usually seen on face especially on cheek and forehead, neck, or on examination similar signs on axillae, groin(all body creases) we clinically think in terms of 'Acanthosis nigricans' due to insulin resistance.
Patients, understandably appear confused when asked to undergo investigations for blood sugar levels and 'I don't have diabetes' is a common response we come across; with a request (demand) for a cream or a procedure to deal with their skin changes. They are not convinced either with the diagnosis or the doctor.
Now when the test results are in, they panic saying they are not diabetic or they do not want medication for diabetes or even not ready to accept that they are in a pre-diabetic state. Counselling the patients regarding insulin resistance is of utmost importance. The task gets tougher in the pediatric and younger age group.
Yes, its common in paediatric and younger age group. Thanks to all the excessive sugars and adulterated dairy products, limitless junk consumption on a daily basis without even realising the harm it's causing to us.
So How do We Deal with this Condition?
Management we offer to these patients focuses on treating insulin resistance as a systemic condition, rather than a localised approach to acanthosis nigricans in isolation.
First step towards treatment is the healthier life: diet modification and regular exercise; 45min daily for at least five times a week. Weight reduction in patients with associated obesity should be achieved by 2-3 kg per month.
Yes, All Doctors Say this; Inspite of having Acanthosis Nigricans and Insulin Resistance How Many Take it Seriously?
Do not assume that the dark thick skin is dirt and try to scrub or rub or go for parlour activities which will only worsen the pigmentation.
Your dermatologist will guide you about application of creams and medication to be taken and counsel you about the wide range of chemical peels available.
Chemical peels being safe, painless and effective usually done once in 6-8 weeks and takes a minimum of 4-6 sessions to appreciate. Total treatment duration varies from 6-8 months
To summarise, insulin resistance is a lifestyle condition with an increasing incidence with acanthosis nigricans being one of its preliminary markers which should be approached as a systemic condition and not just for its cosmetic disfigurement. Treatment options differ from person to person depending on coexisting conditions; however the above options hold good in most of the situations. Results not only depend on the treatment we offer but also on the level of motivation and patient effort.
Insulin Resistance Symptoms
Insulin resistance often progresses without obvious symptoms in its early stages. As the condition advances, subtle clinical signs may begin to appear. Common symptoms may include:
- Persistent fatigue despite adequate rest
- Increased hunger or cravings, especially for carbohydrates
- Difficulty losing weight, particularly around the abdomen with high body mass index (BMI)
- Darkened skin patches in body folds (acanthosis nigricans)
- Fluctuating blood sugar levels in pre-diabetic or diabetic individuals
In addition to these symptoms, insulin resistance is frequently accompanied by metabolic abnormalities such as hypertension (high blood pressure) and hyperlipidemia (elevated blood lipid levels), which are often detected during routine medical evaluation.
Because these symptoms are non-specific, insulin resistance is frequently overlooked unless actively evaluated.
Insulin Resistance Causes
Insulin resistance develops through a combination of genetic, metabolic, and lifestyle-related factors. It is rarely caused by a single issue. Key contributing factors include:
- Excess visceral fat leading to chronic low-grade inflammation
- Physical inactivity reducing glucose uptake by muscles/ high blood sugar levels (glucose toxicity)
- High intake of refined carbohydrates and ultra-processed foods
- Hormonal changes associated with aging or endocrine disorders
- High sodium consumption
- Use of certain medications that interfere with insulin action
- Genetic predisposition affecting insulin signaling pathways
- Elevated circulating fatty acids causing lipotoxic stress
In addition to acquired factors, insulin resistance may occur as part of inherited or syndromic conditions.
Genetic and syndromic causes may include:
- Myotonic dystrophy
- Ataxia-telangiectasia
- Alström syndrome
- Rabson–Mendenhall syndrome
- Werner syndrome
- Lipodystrophy
- Polycystic ovarian syndrome (PCOS)
Long-standing insulin resistance places continuous stress on pancreatic beta cells, accelerating metabolic decline.
Insulin Resistance Risks
Untreated insulin resistance increases the risk of several metabolic and cardiovascular conditions, even before diabetes is diagnosed. Major health risks include:
Common risks associated with insulin resistance include:
- Progression from prediabetes to type 2 diabetes (T2D), as sustained insulin resistance eventually leads to persistent hyperglycemia
- Development of Hypertension (Higher blood pressure), due to impaired vascular regulation and altered sodium handling
- Abnormal lipid levels, including high triglycerides and low HDL cholesterol, increasing cardiovascular risk due to dyslipidemia
- Increased likelihood of non-alcoholic fatty liver disease (NAFLD) due to excess fat accumulation in the liver
- Higher risk of microvascular complications affecting the eyes, nerves, and kidneys
- Elevated risk of macrovascular disease such as coronary artery disease (CAD), stroke, and peripheral artery disease
- Worsening obesity, particularly central fat accumulation, which further amplifies metabolic and inflammatory stress
Recognizing insulin resistance early allows intervention before irreversible metabolic damage occurs.
How to Diagnose Insulin Resistance?
There is no single definitive test for insulin resistance, but diagnosis is based on a combination of clinical assessment and laboratory markers. Evaluation may include:
- Fasting blood glucose and Insulin blood tests
- HbA1c testing to assess long-term glucose trends
- Lipid profile abnormalities suggestive of metabolic dysfunction
- Clinical features such as checking body mass index (BMI) for weight related problems (obesity, sleep apnea, fatty liver, PCOS, or acanthosis nigricans)
- Risk assessment based on family history and lifestyle factors
At PACE Hospitals, diagnosis focuses on identifying insulin resistance before diabetes-related complications develop.
Insulin Resistance Treatment
Management of insulin resistance requires a long-term, individualized approach rather than short-term glucose correction. Treatment strategies focus on:
- Improving insulin sensitivity through regular physical activity
- Nutritional adjustments that reduce glycemic load
- Weight reduction where appropriate
- Eating more fruit and vegetables preferably whole grains
- Avoiding junk food and sugary beverages
- Optimizing sleep and stress management
- Staying away from smoking habit
- Medical therapy when lifestyle changes alone are insufficient
Early and sustained intervention can significantly improve insulin sensitivity and reduce progression to diabetes.
Why Early Action Matters?
Research consistently shows that insulin resistance can be improved—and in some cases partially reversed—when addressed early. Delaying intervention allows metabolic stress to accumulate, increasing the likelihood of diabetes and cardiovascular disease.
At PACE Hospitals, the emphasis is on preventive metabolic care, helping patients understand their risk and take informed steps toward long-term health.
When to Consult a Specialist?
Individuals should seek medical evaluation if they:
- Have prediabetes or fluctuating blood sugar levels
- Struggle with unexplained weight gain or fatigue
- Have a family history of diabetes or metabolic disorders
- Show early metabolic abnormalities on routine testing
Early consultation allows tailored guidance and timely intervention.
Insulin Resistance Care at PACE Hospitals
PACE Hospitals offers a comprehensive approach to insulin resistance that includes:
- Early metabolic screening and risk stratification
- Individualized lifestyle and nutrition counseling
- Medical management when indicated
- Continuous monitoring to prevent disease progression
The goal is not only blood sugar control, but long-term metabolic resilience.
Frequently Asked Questions (FAQs) on Insulin Resistance
How to reverse insulin resistance?
Insulin resistance can often be improved, especially when addressed early. Consistent lifestyle changes such as regular physical activity, weight reduction where appropriate, balanced nutrition, and adequate sleep help restore insulin sensitivity. In some cases, medical therapy may be advised to support metabolic improvement. Reversal is usually gradual and depends on sustained habits rather than short-term measures.
How to check insulin resistance?
Insulin resistance is assessed through a combination of clinical evaluation and laboratory testing. Doctors may review fasting glucose, fasting insulin levels, HbA1c, lipid profile, and metabolic risk factors. There is no single definitive test, so diagnosis focuses on patterns rather than one isolated value.
Why does insulin resistance occur?
Insulin resistance develops when body tissues respond poorly to insulin due to metabolic stress. Factors such as excess visceral fat, physical inactivity, chronic inflammation, genetic predisposition, and hormonal imbalances interfere with insulin signaling. Over time, these disruptions reduce glucose uptake by cells.
Does insulin resistance cause weight gain?
Yes, insulin resistance can contribute to weight gain, particularly around the abdomen. Elevated insulin levels promote fat storage and reduce fat breakdown. This creates a cycle where weight gain further worsens insulin resistance unless interrupted.
Can alcohol cause insulin resistance?
Excessive alcohol intake can worsen insulin resistance by increasing liver fat, inflammation, and metabolic imbalance. Moderate or heavy drinking may interfere with glucose regulation, especially in people already at risk.
Why does insulin resistance occur in PCOS?
In polycystic ovarian syndrome (PCOS), insulin resistance is influenced by hormonal imbalance and genetic susceptibility. Elevated insulin levels worsen androgen excess and disrupt ovulation. Addressing insulin resistance is a key component of PCOS management.
How can insulin resistance be avoided?
Prevention focuses on maintaining metabolic balance. Regular exercise, healthy weight management, balanced meals, stress reduction, and adequate sleep help reduce insulin resistance risk. Early screening in people with family history or metabolic risk factors also play a preventive role.
What should be done for insulin resistance?
Management involves addressing underlying causes rather than focusing only on blood sugar levels. Improving physical activity, dietary quality, and sleep patterns is essential. Medical treatment may be required if lifestyle measures alone are insufficient or if diabetes develops.
Is insulin resistance permanent?
Insulin resistance is not always permanent. Many individuals experience significant improvement with sustained lifestyle changes and appropriate medical care. However, if left unmanaged for long periods, it may progress to irreversible metabolic disease.
What is an insulin resistance diet?
An insulin resistance–friendly diet emphasizes balanced meals with controlled carbohydrate intake, adequate protein, healthy fats, and fiber-rich foods. Reducing refined sugars and processed foods helps stabilize insulin response. Diet plans are best individualized based on metabolic needs.
How does exercise help insulin resistance?
Exercise improves insulin sensitivity by increasing glucose uptake in muscles independent of insulin. Regular physical activity also reduces visceral fat and inflammation. Both aerobic and resistance exercises are beneficial when performed consistently.
How can someone stop being insulin resistant?
Stopping insulin resistance requires long-term metabolic correction rather than quick fixes. Consistent exercise, dietary modification, weight management, and stress control gradually improve insulin signaling. Early intervention yields better outcomes.
Is insulin resistance good?
No. Insulin resistance is a harmful metabolic state that increases the risk of diabetes, cardiovascular disease, and other complications. It represents impaired hormonal efficiency rather than a protective or beneficial process.
Which type of diabetes is insulin resistance associated with?
Insulin resistance is primarily associated with type 2 diabetes. In this condition, insulin is produced but does not work effectively at the tissue level. Over time, insulin production may also decline.
Share on
Request an appointment
Fill in the appointment form or call us instantly to book a confirmed appointment with our super specialist at 04048486868
Appointment request - health articles
Recent Articles










